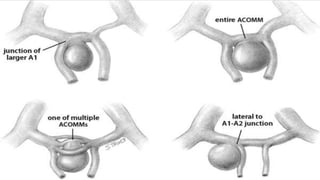
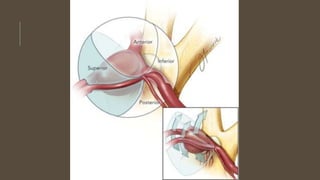
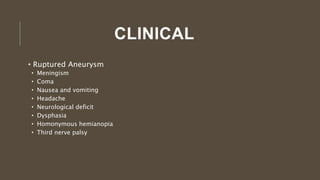
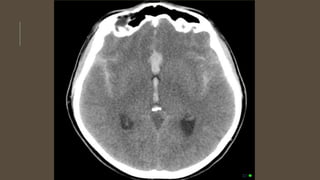
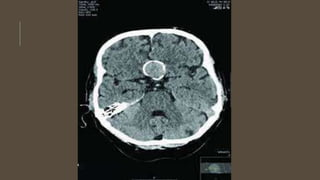
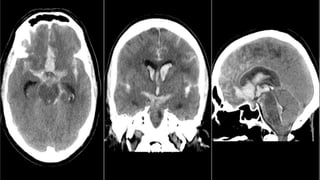
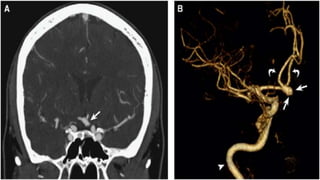
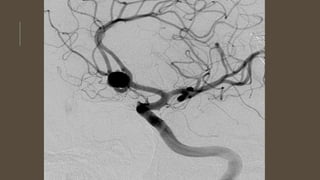
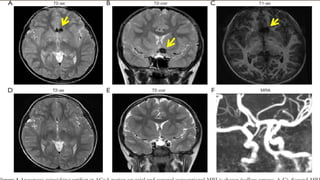
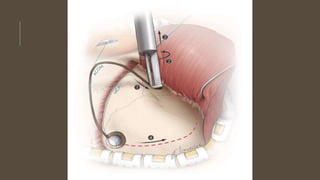
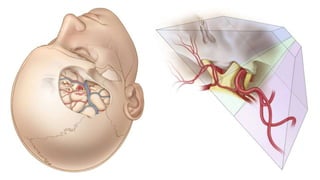
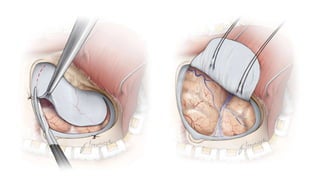
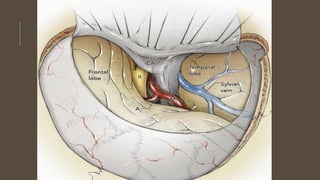
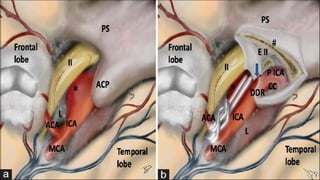
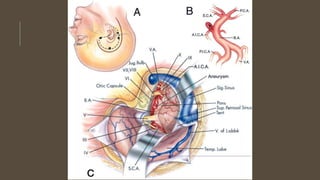
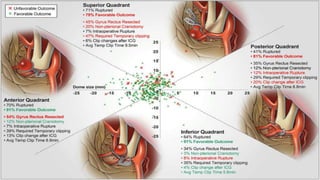
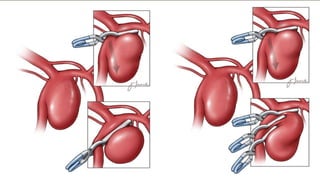
This document outlines the anatomy, causes, clinical presentation, investigations, and management of anterior communicating artery aneurysms. It notes that these aneurysms most commonly occur at the junction of the anterior communicating artery and anterior cerebral artery. Ruptured aneurysms present with subarachnoid hemorrhage, while unruptured aneurysms may cause headaches, visual changes, or neurological deficits. Investigations include CT, MRI, MRA, and DSA. Management involves securing the aneurysm through clipping or coiling to prevent rebleeding, along with treating vasospasm, hydrocephalus, and other complications.