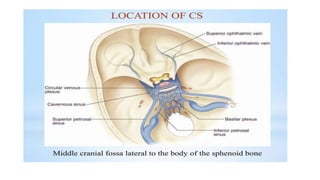
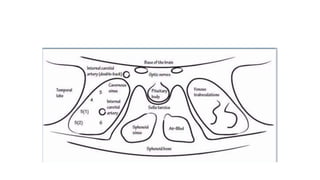
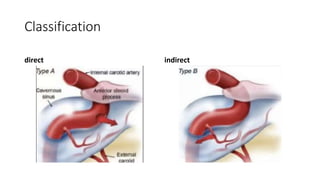
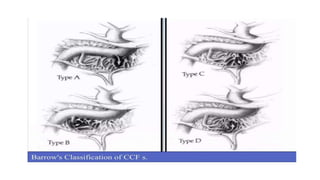
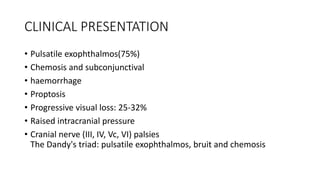
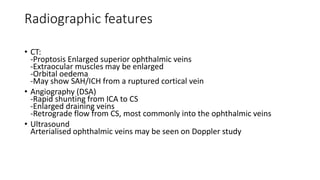
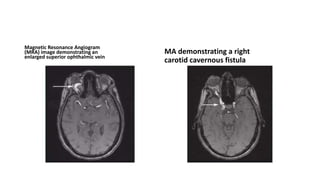
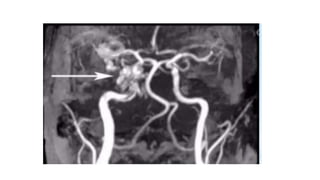
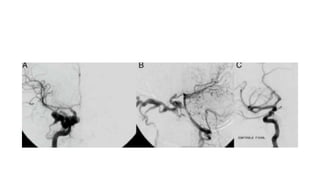
Caroticocavernous fistulas are abnormal connections between the carotid artery and cavernous sinus that result in high pressure arterial blood flowing into the low pressure venous sinus. They can be direct, with a connection to the internal carotid artery, or indirect, involving other meningeal or dural branches. Clinical symptoms include pulsatile exophthalmos, chemosis, and vision issues. Treatment depends on the type of fistula but commonly involves endovascular embolization to occlude the connection using coils or liquid embolic agents via a transarterial or transvenous approach. The goal is to eliminate shunting while preserving arterial patency.