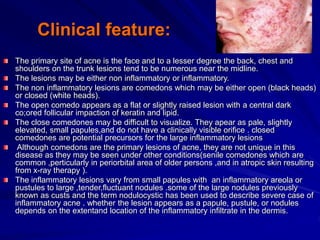
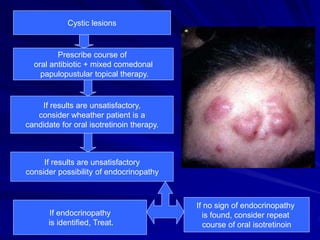
Acne is a chronic skin disease that occurs when hair follicles become plugged with oil and dead skin cells. It usually appears on the face, forehead, chest, and back and is most common in teenagers. The main types of acne lesions include non-inflammatory lesions like comedones and inflammatory lesions such as papules, pustules, nodules, and cysts. Treatment involves topical and oral medications depending on the severity of lesions and may include topical retinoids, benzoyl peroxide, antibiotics, and oral antibiotics or isotretinoin for more severe cases.






















































![Normalisation [Slides].pdf introduction language](https://cdn.slidesharecdn.com/ss_thumbnails/normalisationslides-241027214218-f965ea10-thumbnail.jpg?width=640&height=640&fit=bounds)
![Logic operators [Slides].pdf introductory](https://cdn.slidesharecdn.com/ss_thumbnails/logicoperatorsslides-241027214044-f1a65760-thumbnail.jpg?width=640&height=640&fit=bounds)
































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




