Download as PDF, PPTX

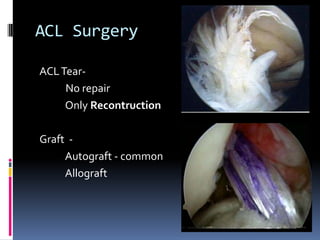

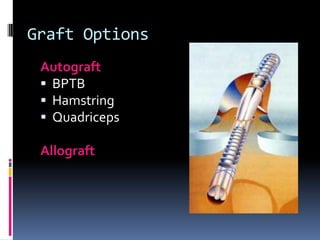
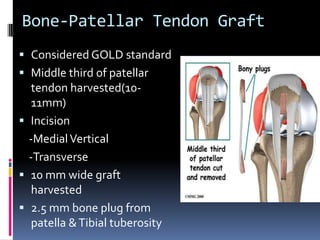


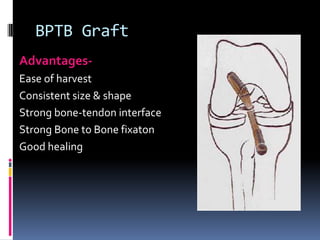
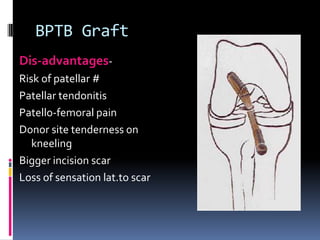




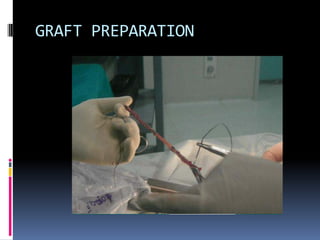

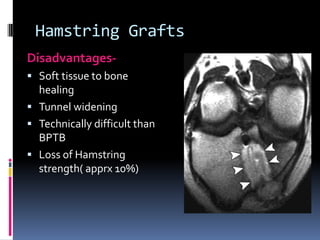
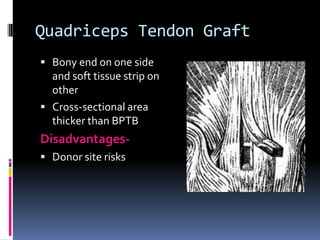
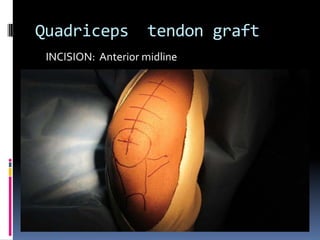




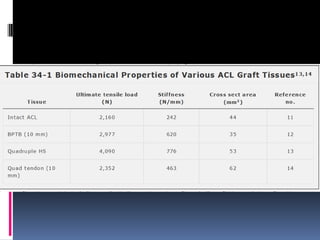












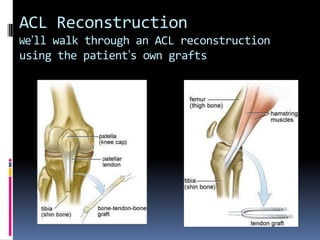
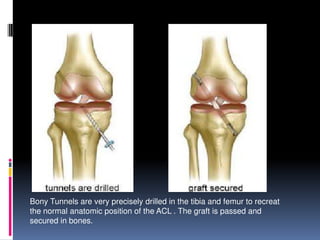
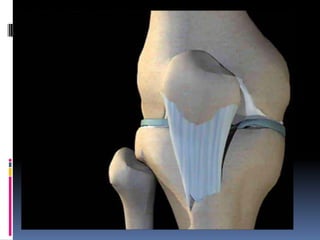
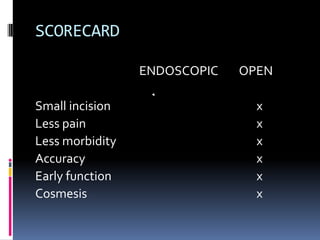

The document discusses ACL reconstruction options, emphasizing graft types such as autografts (BPTB, hamstring, quadriceps) and allografts, along with the importance of proper tunnel placement and fixation techniques for successful outcomes. It details the advantages and disadvantages of each graft type, surgical techniques, and post-operative considerations, highlighting the need for accurate surgical methods to prevent complications. Additionally, it notes that autografts generally provide better results than allografts and stresses the significance of appropriate fixation methods for rehabilitation.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







