Downloaded 331 times
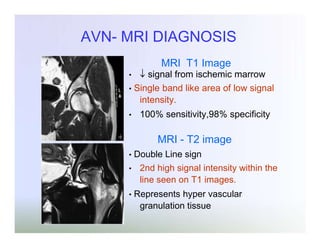
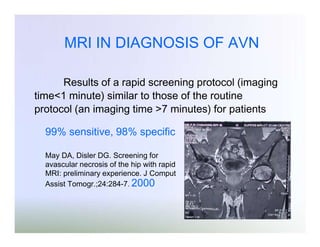
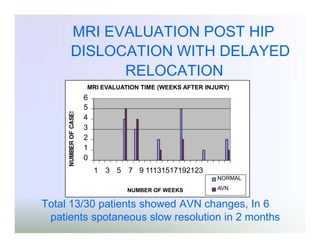
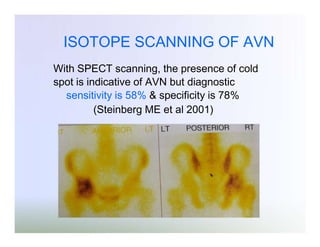

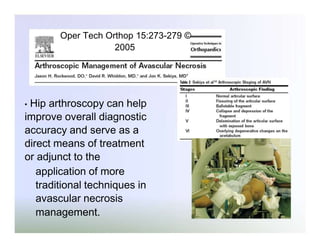
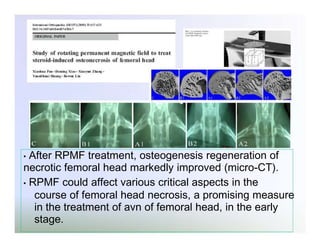
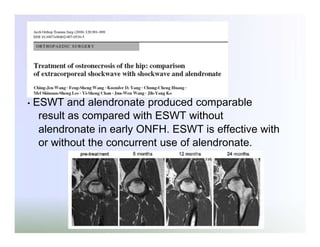
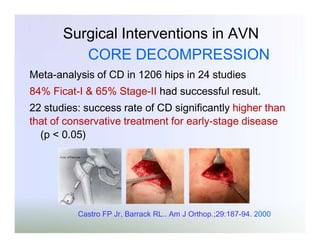
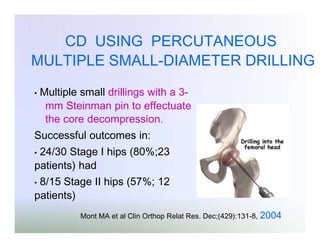

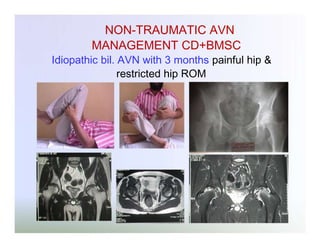
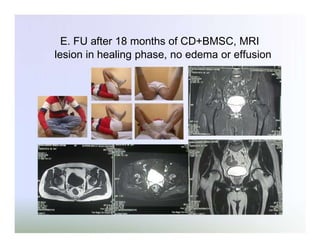

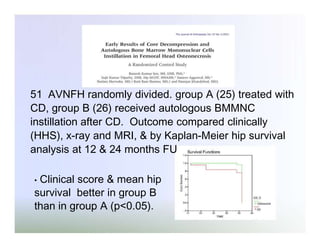
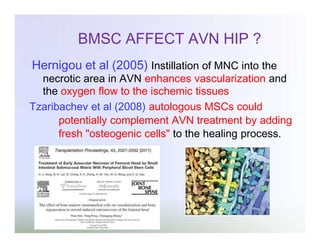
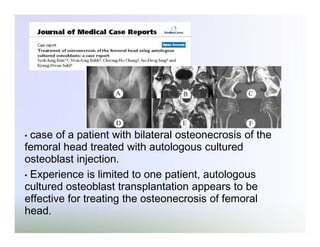



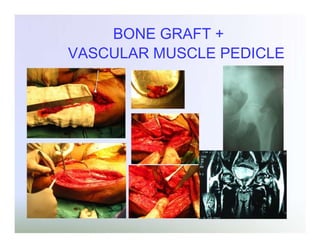
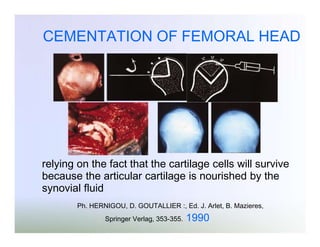
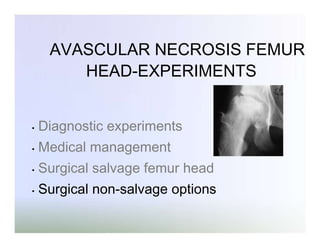

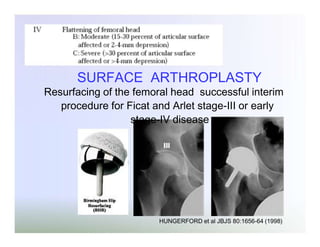


This document summarizes experiments on avascular necrosis of the femoral head. It discusses diagnostic experiments including MRI diagnosis and isotope scanning. It also discusses non-surgical interventions such as restricted weight bearing, pharmacological agents, hyperoxygenation, bisphosphonates, and core decompression with adjunct therapies. Surgical interventions discussed include core decompression, core decompression with bone morphogenetic protein and autologous bone marrow, and total hip replacement for advanced cases.































































































