Download to read offline




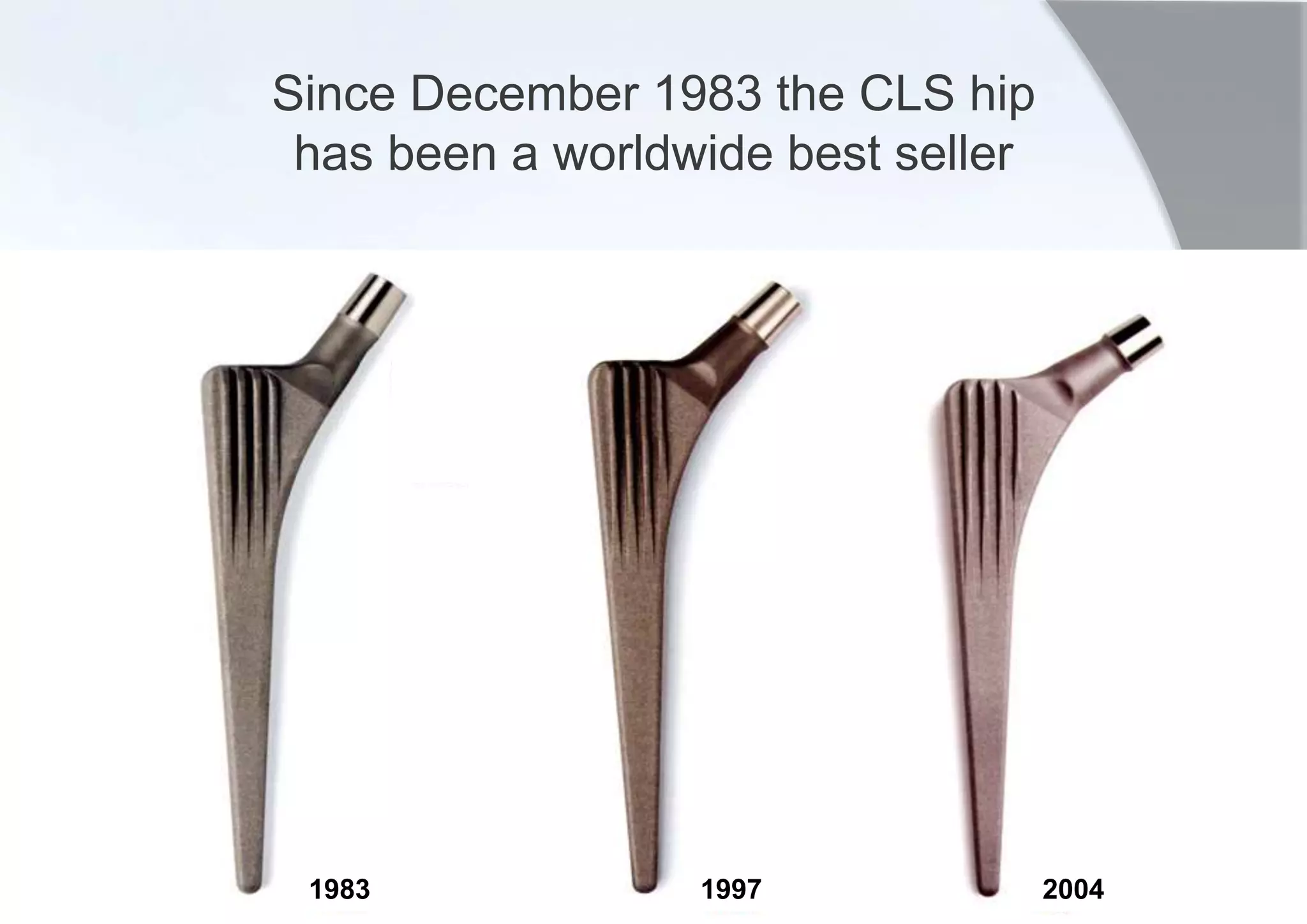
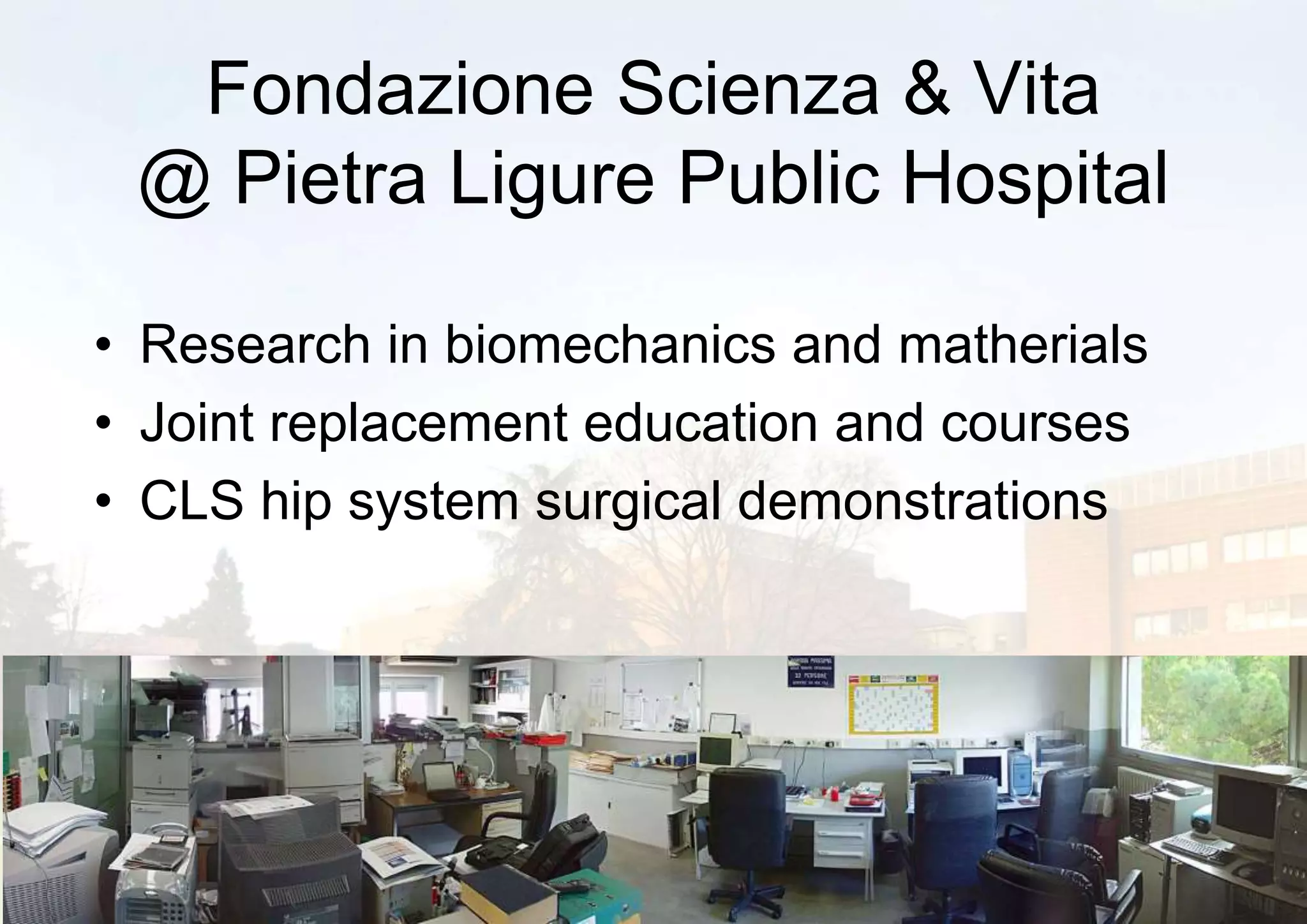


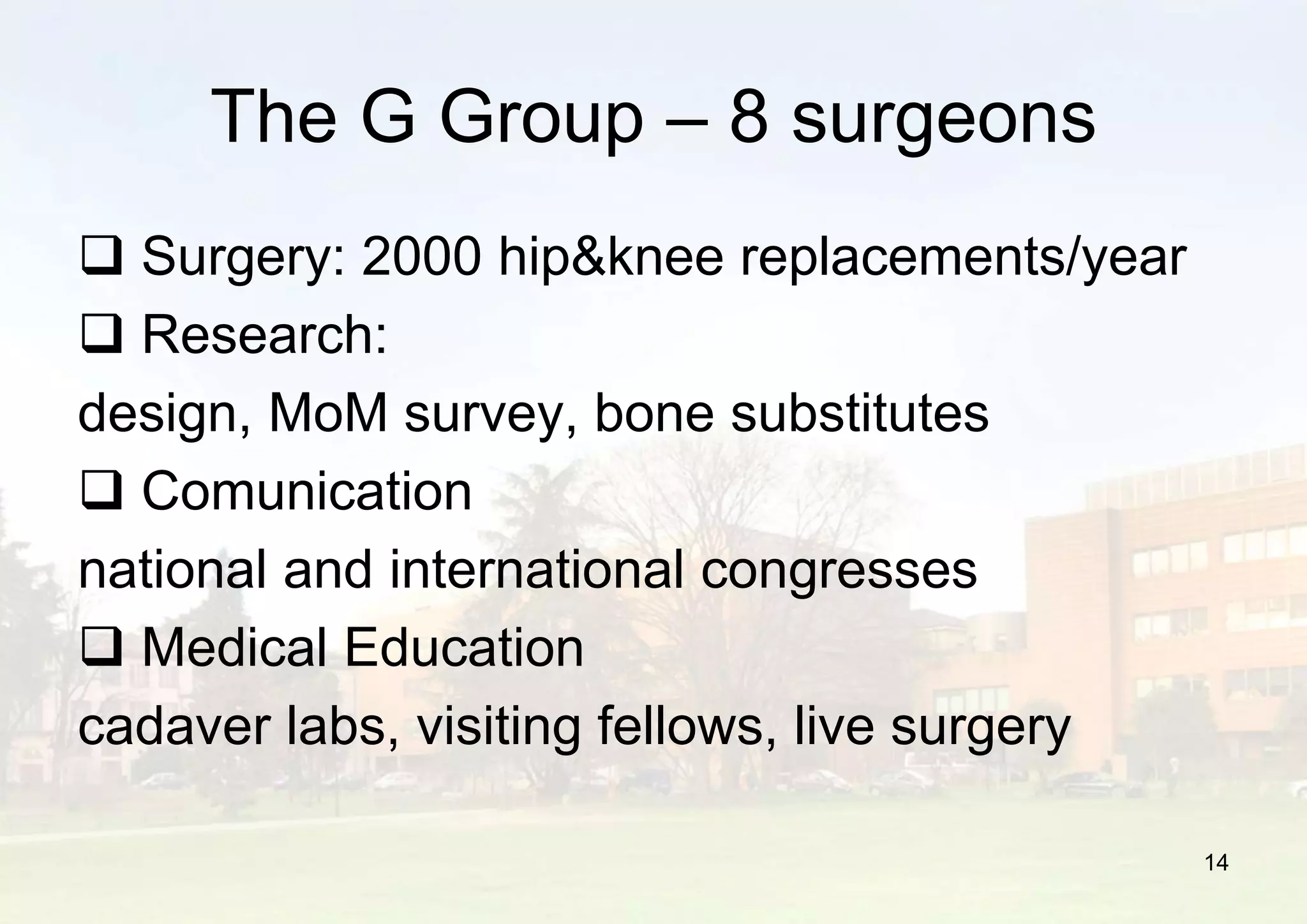

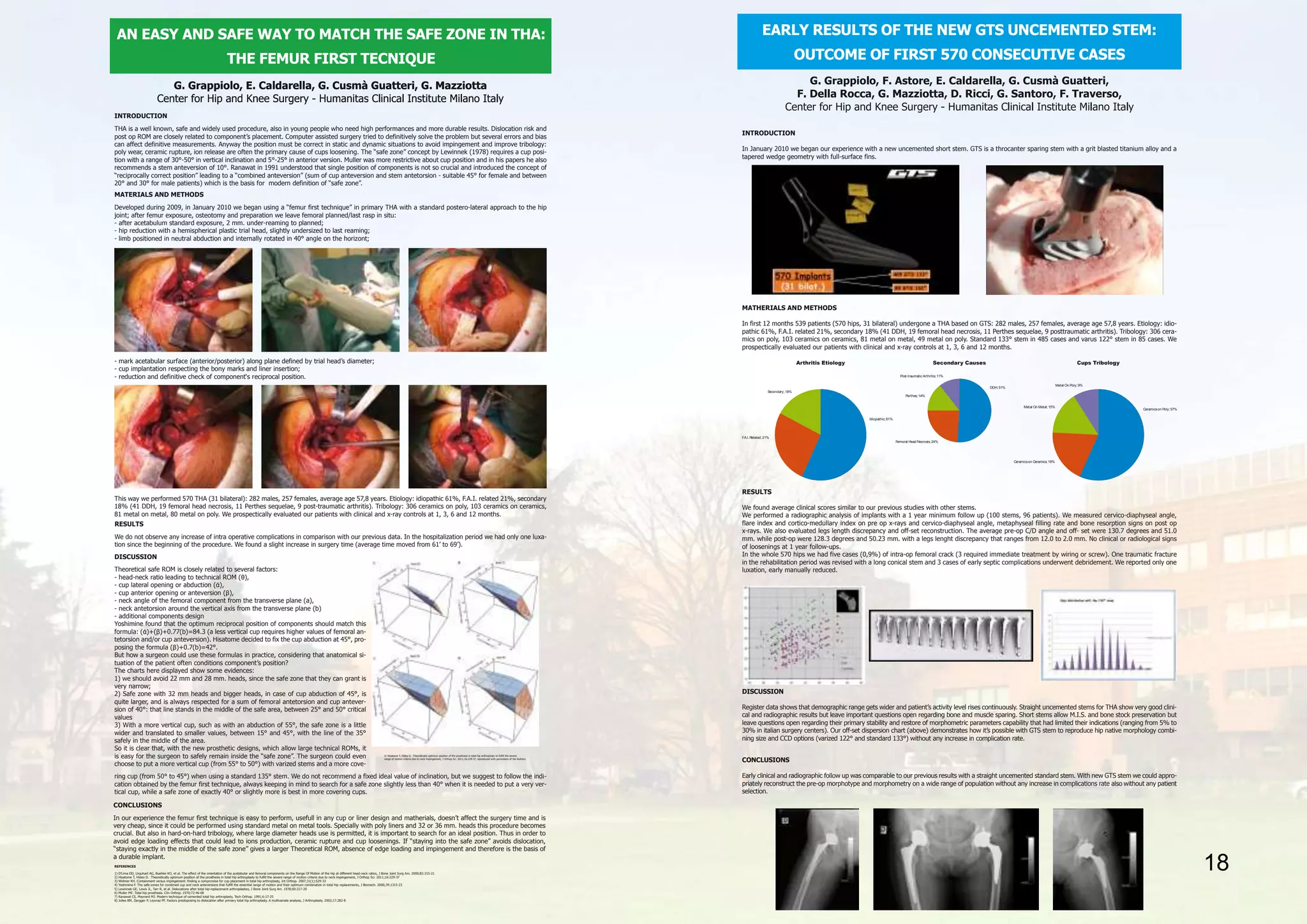





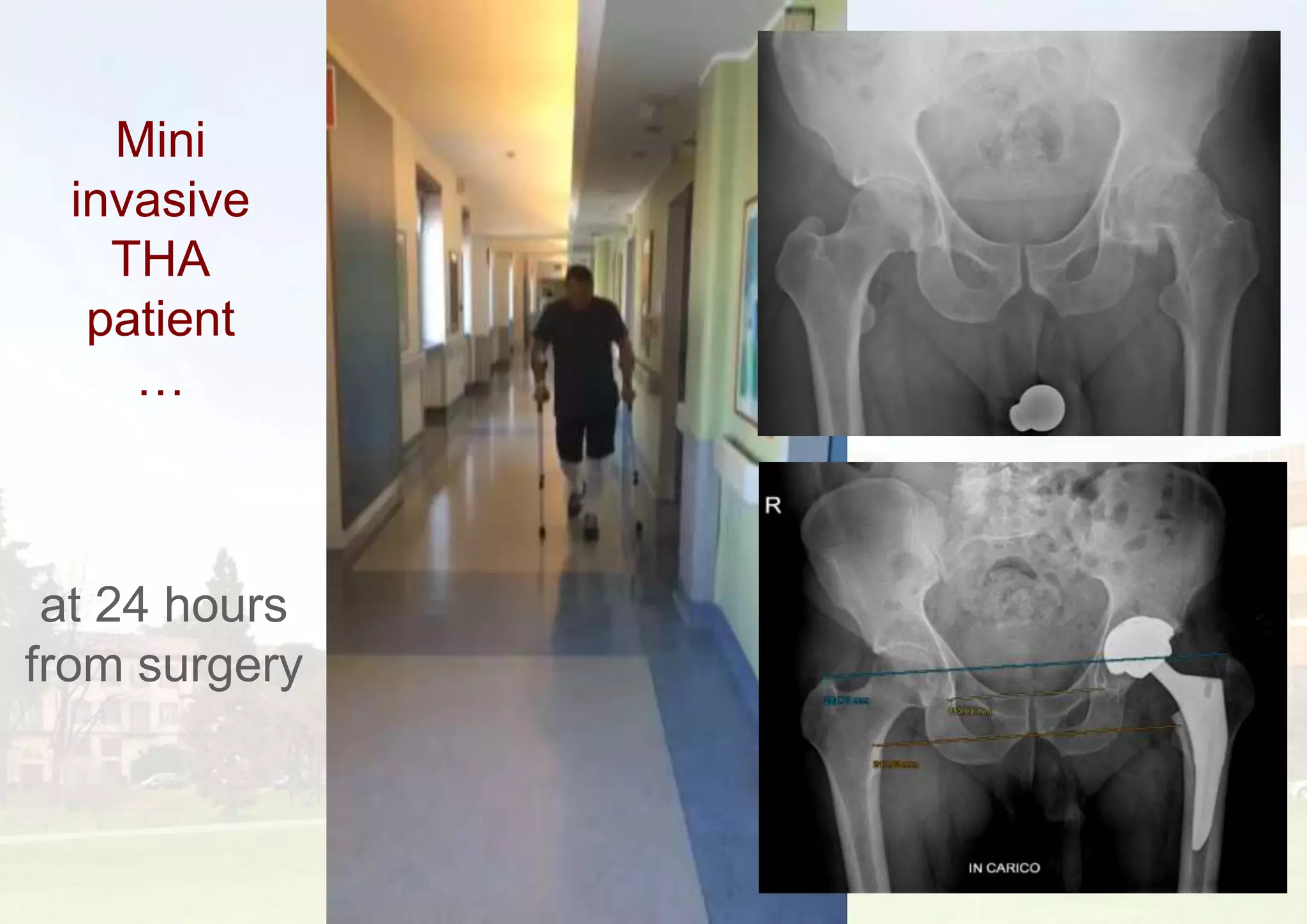

This document provides information about hip and knee replacement services at Humanitas Research Hospital in Italy. It discusses the history and founding of hip replacement research and education centers in Pietra Ligure and Rozzano led by Prof. Lorenzo Spotorno and Prof. Guido Grappiolo. It highlights the hospital's high volume of joint replacements per year, focus on research and education, and use of innovative techniques like fast track recovery programs and mini-invasive surgeries. Early results with a new uncemented short stem hip implant called GTS are also summarized, showing outcomes comparable to previous implants.
































































