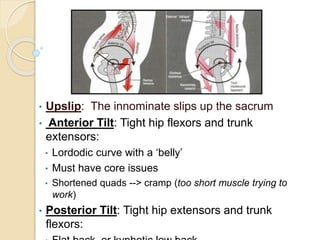
This document discusses assessing and addressing pelvic alignment issues. It describes three types of pelvic tilt: upslip, anterior tilt, and posterior tilt. Multiple assessment techniques are provided to analyze the pelvis, including examining iliac crests, PSIS bones, leg length, and posture. Self-mobilization and manual techniques are presented to address specific tilts. Maintaining core stability and balanced hip strength through regular exercise is emphasized for retaining proper pelvic alignment.