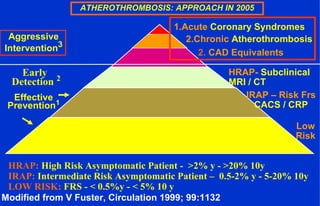
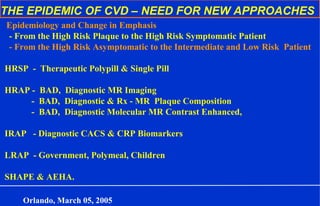
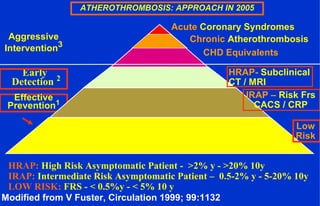
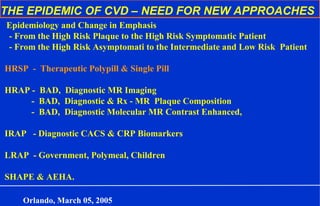
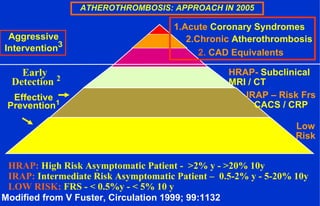
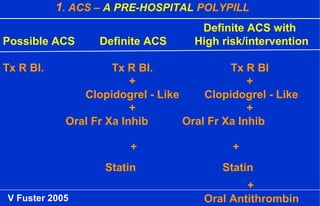
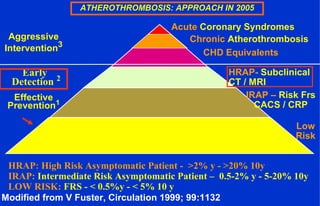
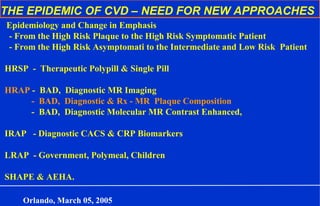
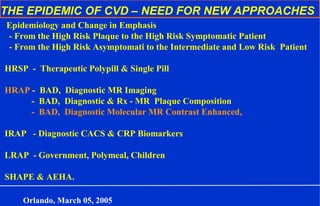
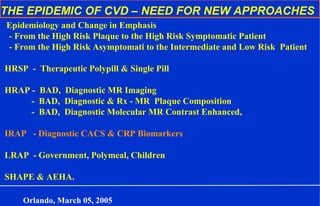
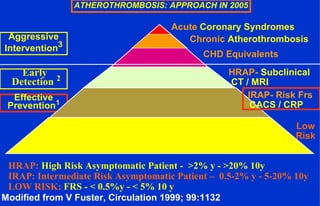
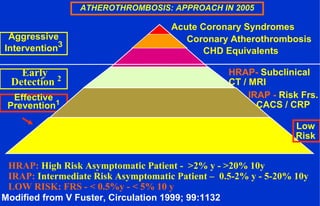
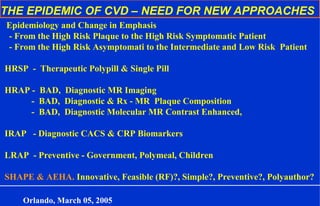
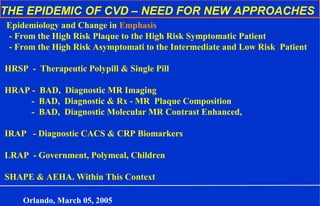
This document discusses approaches to cardiovascular disease (CVD) and the need for new approaches. It summarizes that the emphasis is shifting from high risk plaques to high risk symptomatic patients, and from high risk asymptomatic to intermediate and low risk patients. It discusses diagnostic tools like magnetic resonance imaging to identify high risk asymptomatic patients and computed tomography to identify intermediate risk patients using coronary artery calcium scoring and CRP biomarkers. It also discusses prevention and treatment strategies like a polypill for acute coronary syndrome patients and those with chronic atherothrombosis.






























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















