
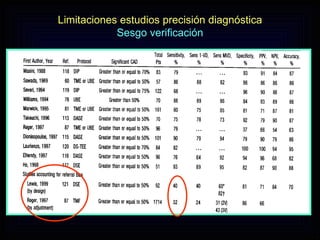
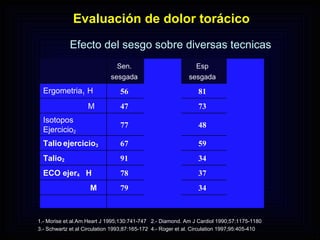
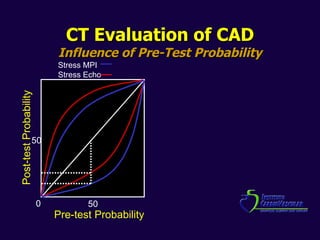
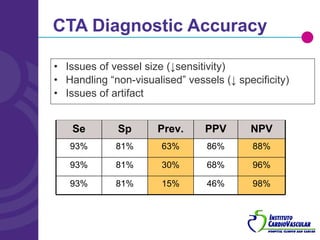
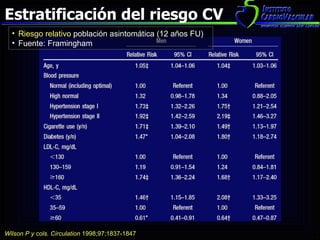
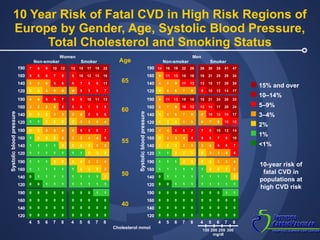



The document discusses non-invasive coronary disease evaluation techniques, emphasizing the limitations and biases in diagnostic accuracy. It highlights the importance of pre-test probabilities and various imaging modalities such as CT and echocardiography in identifying significant coronary artery disease. The text also addresses the need for advanced strategies to detect high-risk patients to improve cardiovascular outcomes.









































































































