Downloaded 51 times







![ Direct in vivo measurement of thickness of carotid
artery wall by B-mode ultrasound
Vessel wall thickness correlates with status of
atherosclerosis and CV events
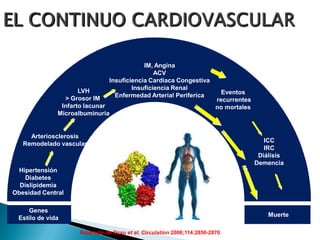
Atherosclerosis is a systemic disorder
◦ Atherosclerosis in the carotid artery is predictive of disease in
other vascular beds
de Groot E, et al. Circulation. (2004) 109[Suppl III]:III-33-III-38.](https://image.slidesharecdn.com/riesgocardiometaboliconov2012-130806083411-phpapp02/85/RIESGO-CARDIOMETABOLICO-52-320.jpg)


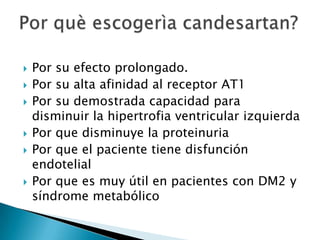

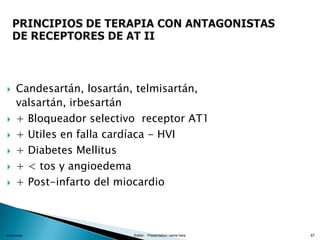
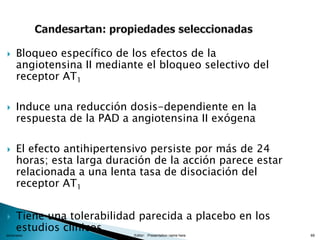


Los fármacos recomendados para iniciar el tratamiento antihipertensivo en este paciente son: - Candesartán: por su demostrada capacidad para disminuir la hipertrofia ventricular izquierda y reducir la proteinuria, lo que es importante dado que el paciente presenta diabetes e hipertrofia ventricular. - Telmisartán: al igual que el candesartán, ha demostrado reducir la proteinuria en pacientes diabéticos. Además, posee efecto antioxidante y antiaterogénico que son beneficiosos en este tipo de pacientes. - V























































![Nuevasguiasdislipidemia2018 [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/nuevasguiasdislipidemia2018autoguardado-190507175428-thumbnail.jpg?width=640&height=640&fit=bounds)































