
Download to read offline

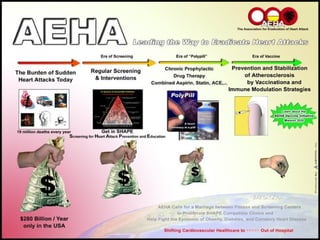

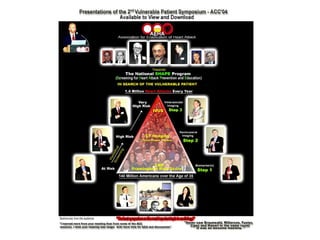
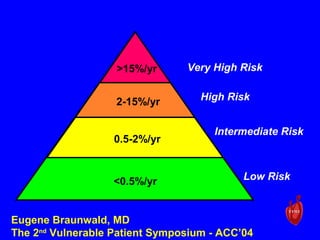
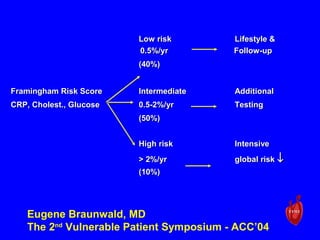
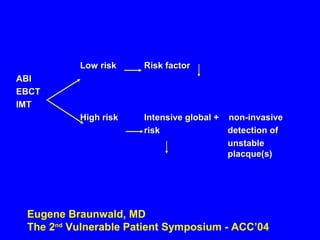
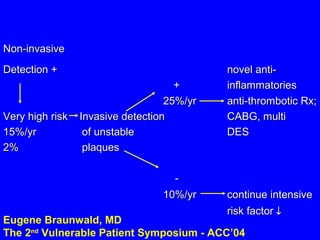
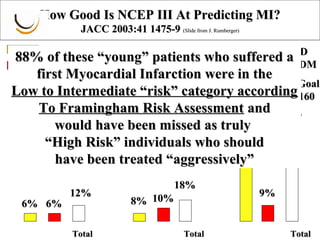
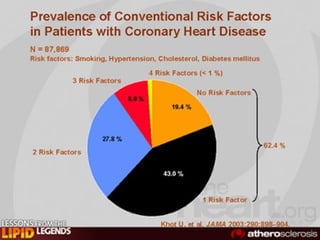
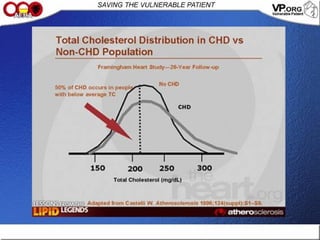
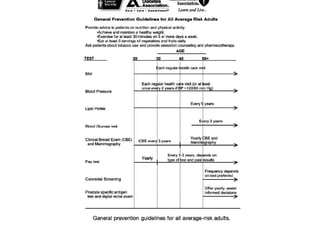
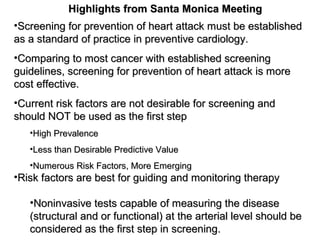
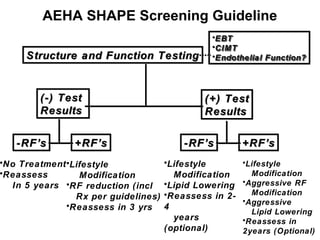
This document discusses the need for screening and prevention of acute cardiovascular events. Some key points discussed are: - Prevention of acute events through screening must be the primary goal of preventive cardiology, rather than treatment after the fact. - Current risk factor approaches are not ideal for screening purposes due to their limited predictive value and numerous emerging risk factors. - Noninvasive tests capable of measuring arterial disease through structure and function should be considered as the first step in screening, rather than risk factors alone. - Over 140 million Americans have high cholesterol or average risk, and 76.5 million have high CRP, highlighting the need for improved screening approaches.








































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
