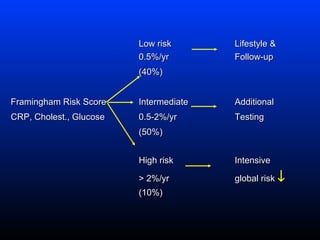
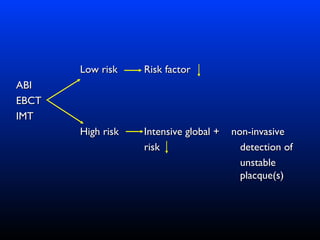
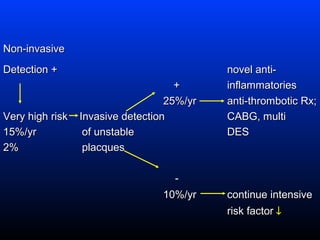
This document discusses approaches to identifying and managing coronary risk. It states that the primary goal should be preventing acute cardiac events through intensive risk factor reduction for all patients with clinically apparent heart disease. Additionally, it notes that one third of sudden cardiac deaths and heart attacks occur in previously asymptomatic individuals with undiagnosed risk factors or pre-clinical disease. The document proposes identifying high-risk asymptomatic individuals through testing to provide prevention. It presents a risk stratification approach using testing like CRP, cholesterol, glucose and imaging to guide different levels of risk factor reduction and management.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















