
Download to read offline



![Circulation. VP Consensus Document. 2003 Oct 7;108:1664-72Circulation. VP Consensus Document. 2003 Oct 7;108:1664-72
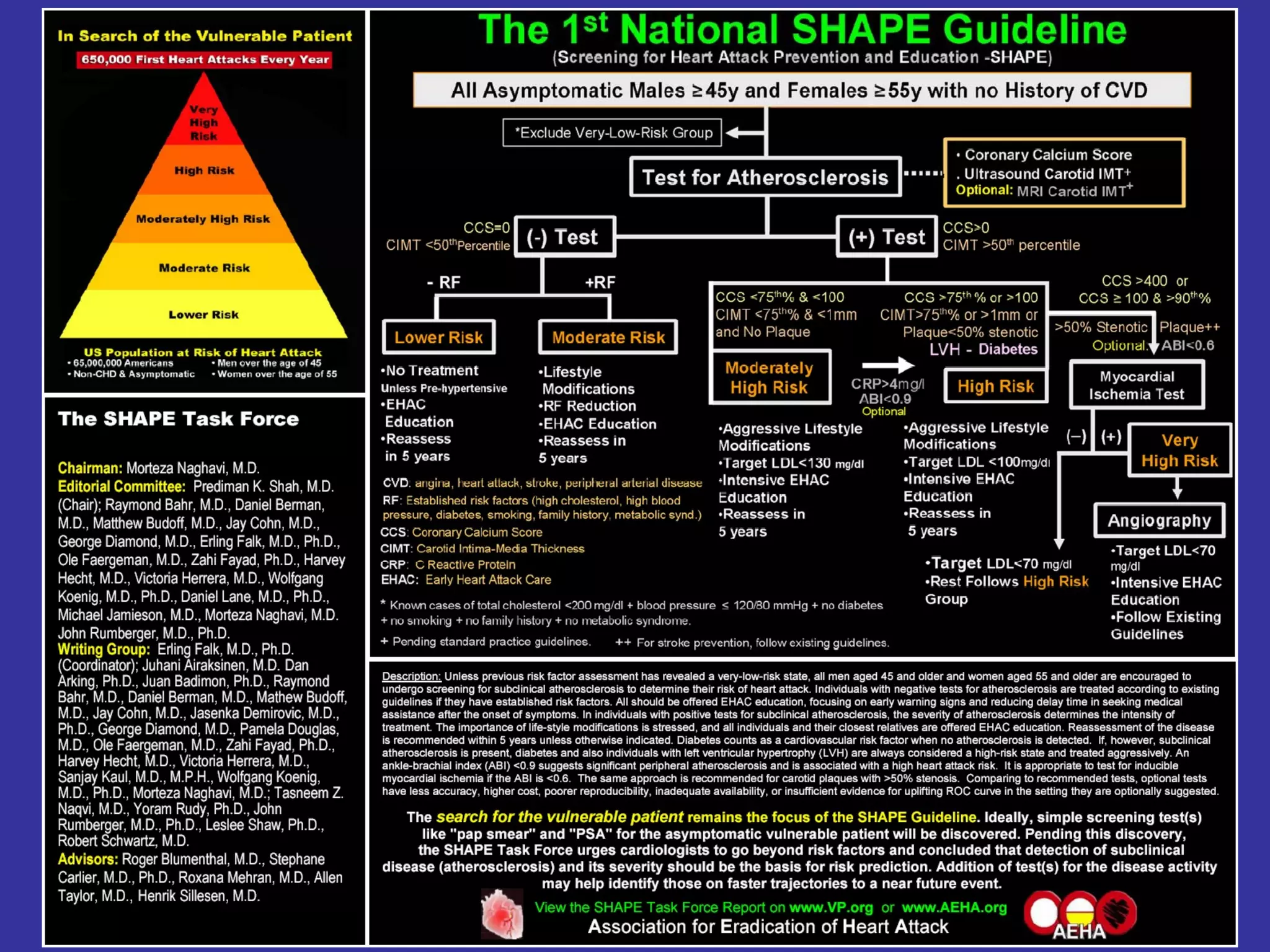
Vulnerable plaque (Part I)
+ Vulnerable blood & myocardium (Part II, Oct 14)
→ Vulnerable patient: high risk of near-term (Part III)
From:From: Morteza NaghaviMorteza Naghavi , M.D. [mailto:mn2@vp.org], M.D. [mailto:mn2@vp.org]
Sent:Sent: Tue 3/1/2005 2:26 AMTue 3/1/2005 2:26 AM
… in case of symptomatic or post-ACS population we all know the
balance between components of vulnerability (i.e. plaque – blood –
myocardium) shifts toward increasing the role of blood and
myocardium.](https://image.slidesharecdn.com/jk4xpg8eru6oq9yu0fa1-signature-ff2318a174bfd4e5f1d417a23528cae62d8d53b9035de413ac0871ada57f583e-poli-160914033507/85/Dr-falk-s-slides-part-i-21-320.jpg)
![From: Morteza Naghavi, M.D. [mailto:mn2@vp.org]
Sent: Thu 2/24/2005 7:47 AM
To: Erling Falk; John Rumberger; Kaul, Sanjay M.D.; HHecht@aol.com; Kaul, Sanjay M.D.; Diamond, George, MD
Cc: lshaw@acrionline.org; Kaul, Sanjay M.D.; JamieM@pfizer.com; Dmlmdphd@aol.com; Jasenka.Demirovic@uth.tmc.edu;
Shah, Prediman Krishan
Subject: RE: Association vs classification
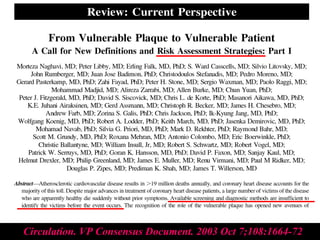
Let's not forget the most important question, the short-
term prediction (<5y) in search of the Vulnerable Patient.
We didn't start SHAPE just to engineer a new paradigm. The concept of
search for the Vulnerable Patient, those at a very high risk of a near term
event is by itself a new paradigm and requires new approaches. Preventive
cardiology today does not have any recognition for this group and put them all
together with high risk. ……](https://image.slidesharecdn.com/jk4xpg8eru6oq9yu0fa1-signature-ff2318a174bfd4e5f1d417a23528cae62d8d53b9035de413ac0871ada57f583e-poli-160914033507/85/Dr-falk-s-slides-part-i-33-320.jpg)
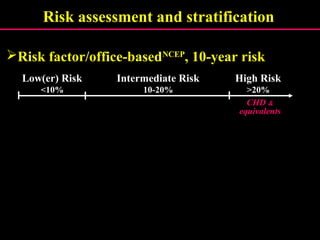
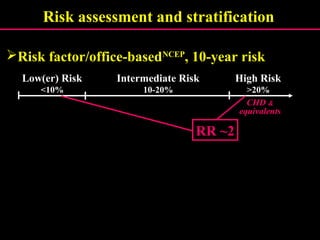
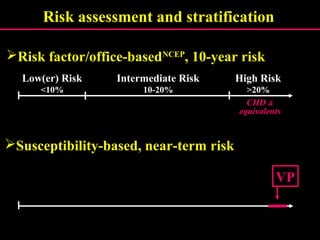
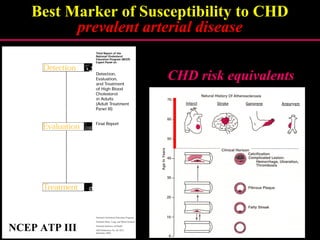
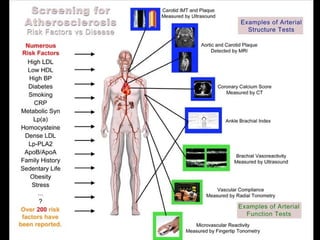
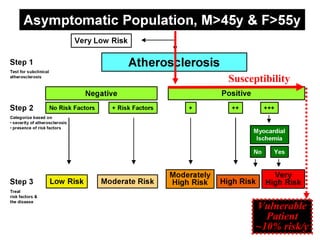
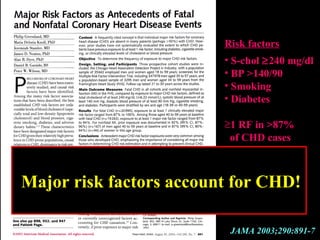
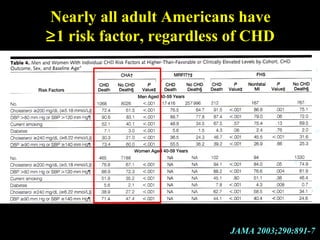
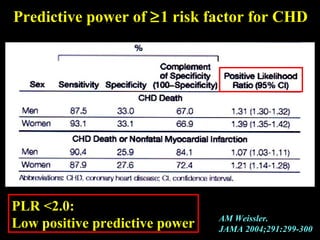
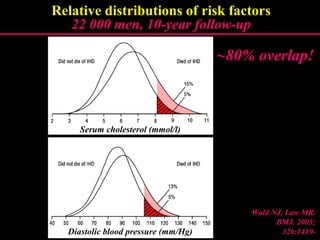
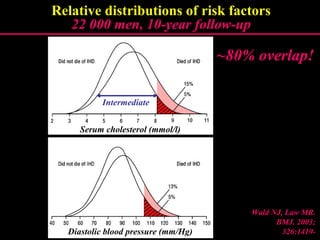
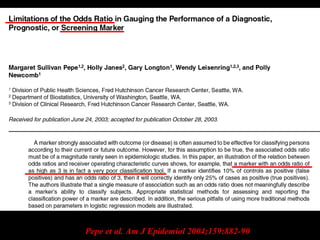
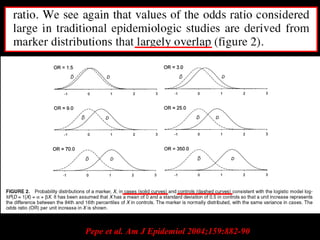
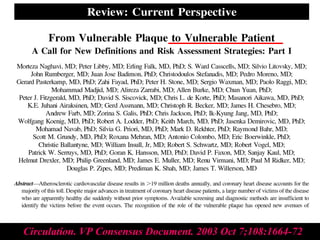
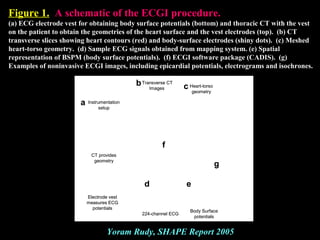
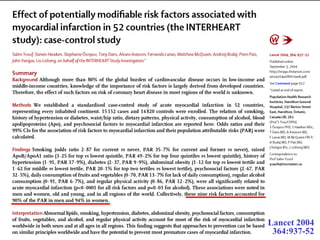
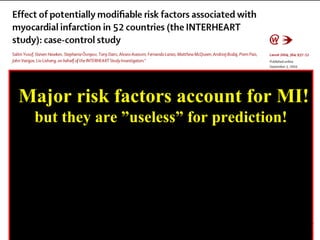
This document contains an expert's curriculum vitae focusing on vulnerable plaques, coronary thrombosis, and acute coronary syndrome. It lists his main interests and publications on related topics. It also discusses risk factors for coronary heart disease, limitations of current predictive models, definitions of vulnerable patients with high short-term risk, and the need for new approaches to identify those most susceptible to near-term cardiac events.



































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















