Downloaded 149 times



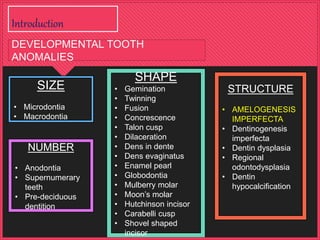
















































(1) The document discusses amelogenesis imperfecta (AI), which refers to hereditary defects in enamel formation. It describes several classifications of AI based on clinical, radiographic, and histological findings. (2) The main types are hypoplastic (reduced enamel), hypocalcified (soft enamel), and hypomaturation (improperly formed enamel). Clinical features, inheritance patterns, and prevalence are provided for each type. (3) The case report describes a 26-year-old female patient diagnosed with hypoplastic AI based on yellow-brown tooth discoloration and decreased vertical dimension. She was treated with periodontal therapy and full-mouth fixed bridges.

















































































