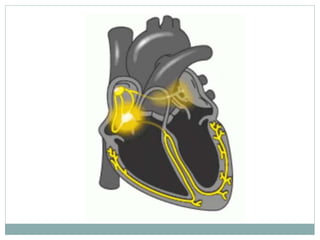
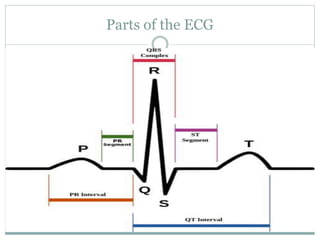
The document provides information about electrocardiograms (ECGs), including a brief history of ECG development, basic cardiac anatomy and the heart's conducting system, components of the ECG waveform, electrode placements, how to read ECG paper, and cardiac axis. It explains that the ECG is a tool that records electrical activity of the heart to assess cardiac function and identify abnormalities, traces its development back to Willem Einthoven in the 1890s, and provides details on heart structures involved in the cardiac cycle and what different parts of the ECG represent.
























































![ECG [electrocardiogram].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ecgelectrocardiogram-220416062706-thumbnail.jpg?width=640&height=640&fit=bounds)
































