Downloaded 33 times
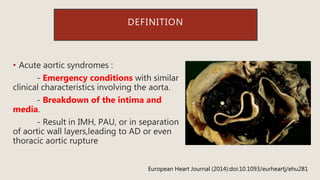
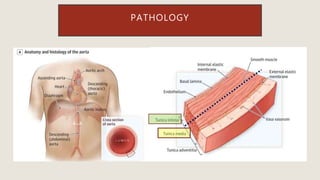
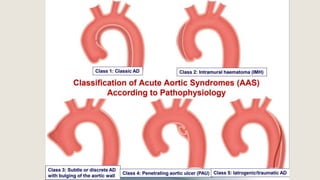
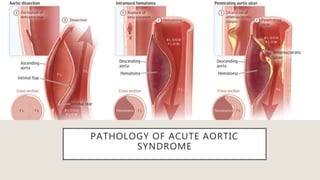
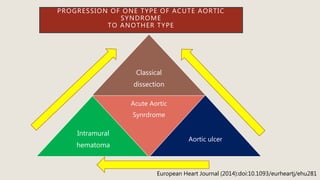
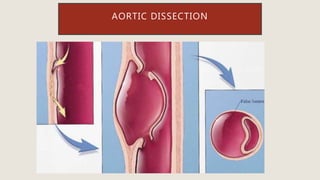
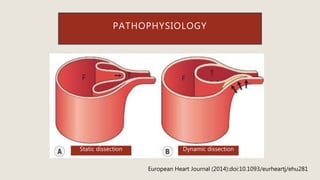
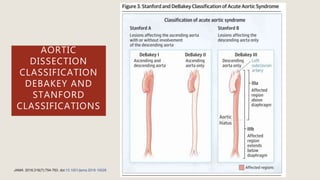
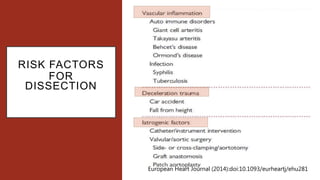
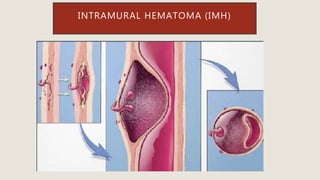
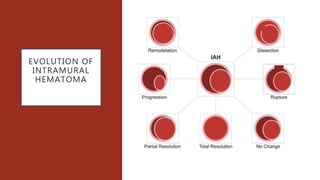
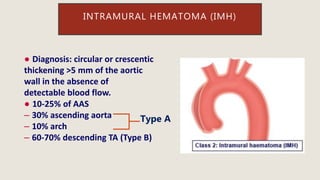
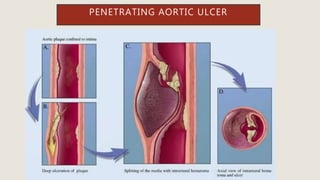
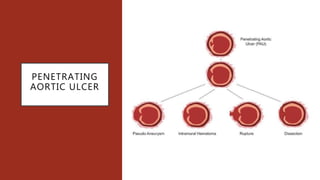
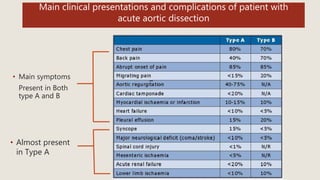
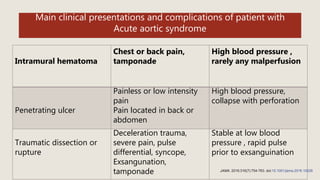
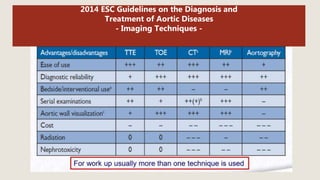
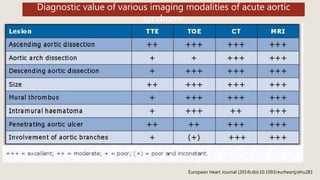
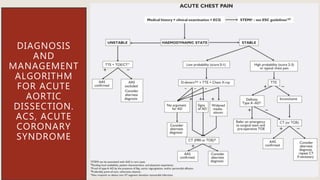
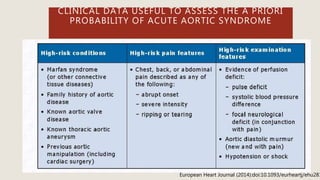
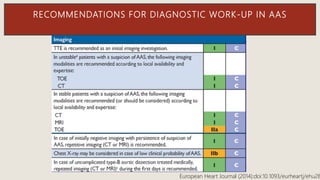
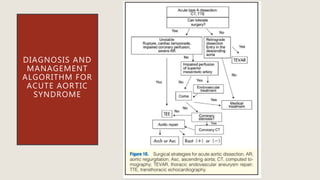
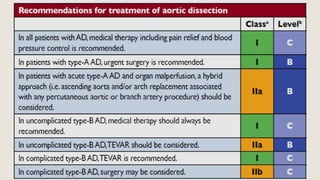
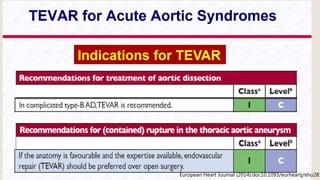
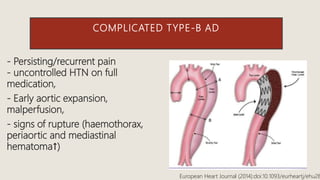
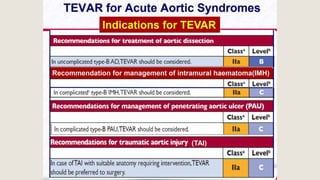
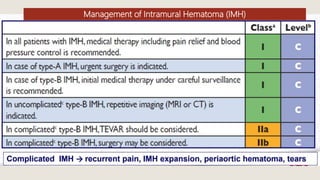
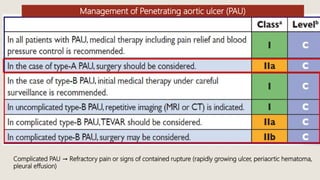
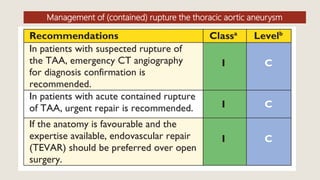
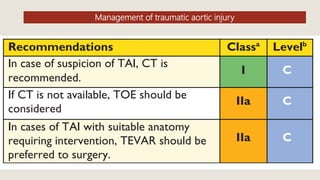
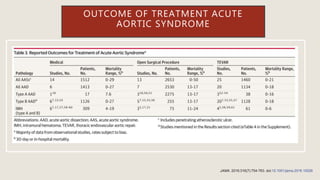
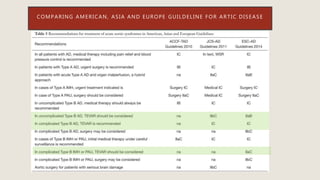
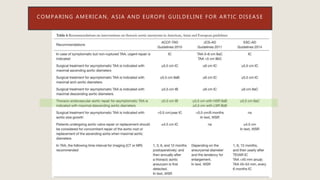

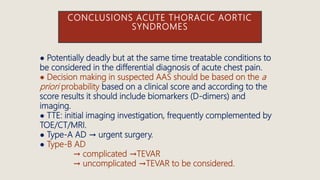


Acute aortic syndromes include aortic dissection, intramural hematoma, and penetrating aortic ulcer. They involve a breakdown of the aortic wall layers. Type A dissection requires urgent surgery while type B can be managed medically or with TEVAR for complications. Intramural hematoma and penetrating ulcers are generally treated medically but TEVAR is considered for complications. Guidelines provide algorithms for diagnosis and management based on syndrome type, complications, and patient factors. TEVAR has become preferred over surgery for some conditions when anatomy is favorable.