Download to read offline








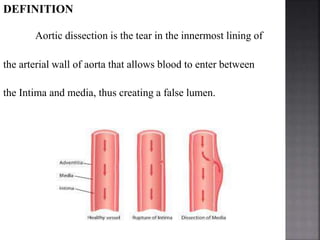

































A 45-year-old man presented to the emergency department with severe chest pain radiating to his back for 2 hours. His vital signs showed elevated blood pressure and absent radial pulses. An ECG showed sinus tachycardia but no signs of ischemia. A chest x-ray revealed a widened mediastinum. He was initially stabilized and transferred to the CCU for further investigation and management, which may include aortic dissection. Aortic dissection involves a tear in the inner layer of the aorta allowing blood to flow between the layers, and can be classified and treated in different ways depending on its location and severity.


































































