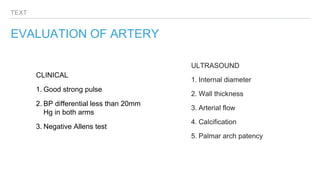
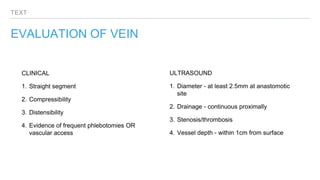
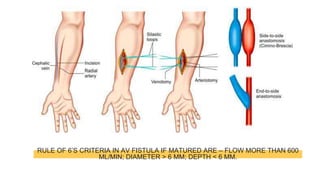
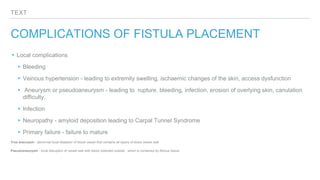
The document discusses arteriovenous (AV) fistulas for hemodialysis access. It describes the need for well-perfused venous access in end-stage renal failure patients undergoing hemodialysis. The optimal location is a distal forearm fistula that is superficial, straight, and has adequate blood flow of at least 500-700 cc/min. The document outlines guidelines for fistula creation timing and types including radiocephalic, brachiocephalic, and grafts. It provides details on patient evaluation, surgical strategy, maturation criteria, complications, and post-operative care of AV fistulas.














































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


