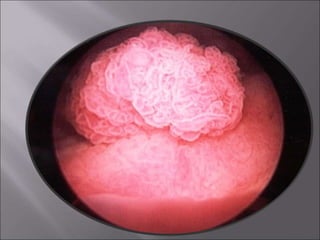
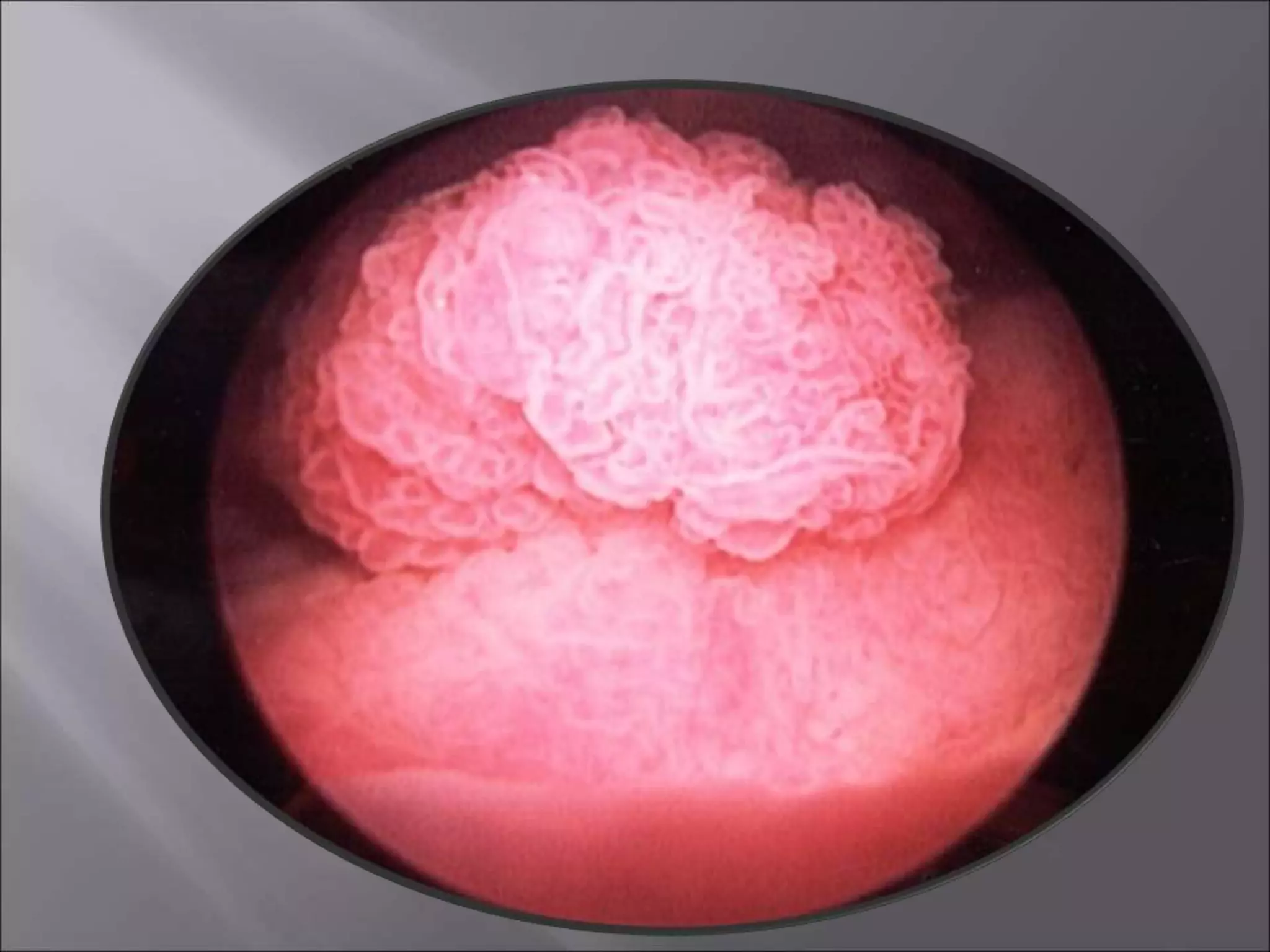
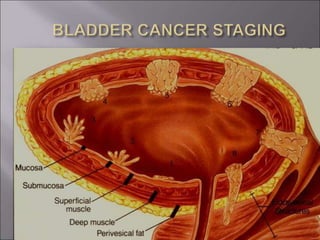
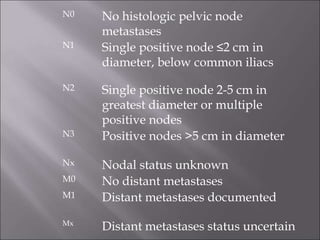
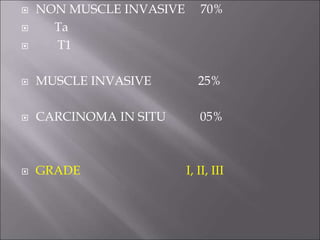
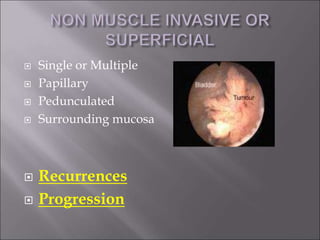
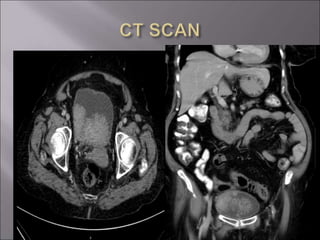
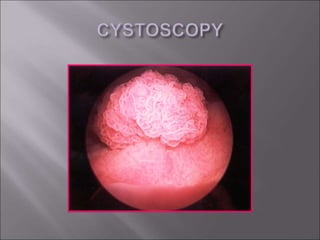
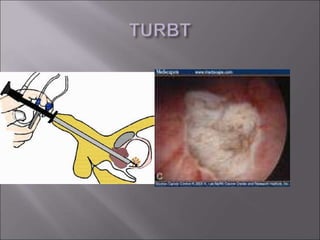
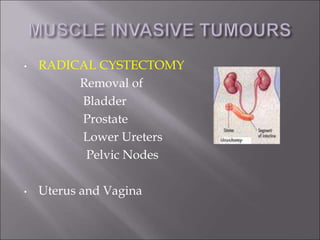
This document discusses transitional cell carcinoma of the bladder. It notes that 90% of bladder cancers are transitional cell carcinoma, while 5% are squamous cell carcinoma and 1% are adenocarcinoma. It covers causes, staging according to the TNM system, types of bladder tumors, behavior, symptoms, investigations, and treatments which include transurethral resection of the bladder tumor (TURBT) for non-muscle invasive tumors and radical cystectomy for muscle-invasive tumors. Recurrence rates are higher for carcinoma in situ, high grade tumors, and those with a high chance of recurrence, so intravesical BCG may be used after TURBT for these cases.