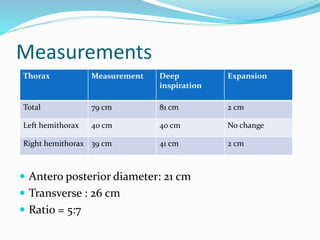
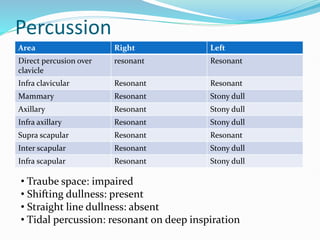
A 43-year-old female homemaker presents with 15 days of fever, chest pain, and breathlessness, with a diagnosis of moderate left-sided pleural effusion likely due to tuberculosis. General examination reveals no significant abnormalities aside from respiratory distress and reduced left hemithorax movement. The patient will be treated with antibiotics, tuberculosis management, and possibly drainage of the pleural fluid.











![[MBBS/MS/DNB] Sample EXAM Long Case on Breast Lump](https://cdn.slidesharecdn.com/ss_thumbnails/cccbreast-200518145117-thumbnail.jpg?width=640&height=640&fit=bounds)









































































