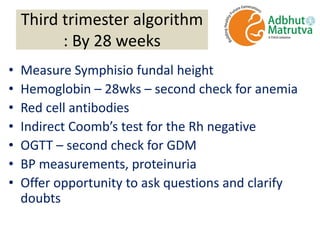
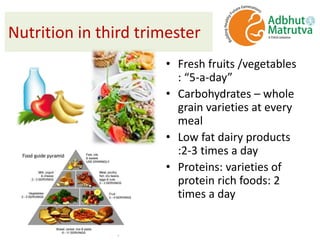
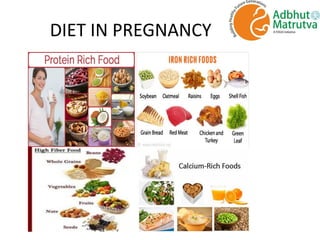
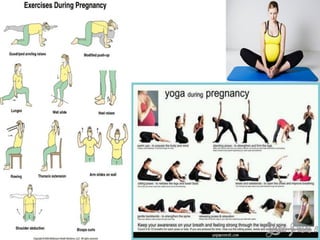
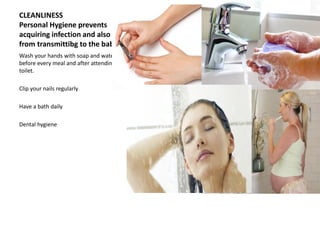
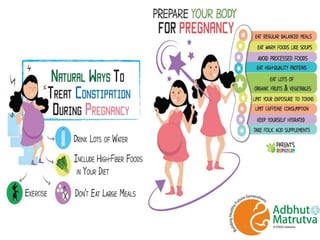
Dr. S. Shantha Kumari presents an algorithmic approach for antenatal care during the third trimester of pregnancy from 28 weeks until labor and delivery. The algorithm proceeds in a step-by-step logical manner, reviewing past medical history and tests from the second trimester, and outlining checks and interventions to be completed at various gestational ages including nutrition, exercises, mental preparation, and monitoring for signs of preterm labor or other complications. The overall goal is to provide timely, evidence-based care that reduces risks and promotes a healthy pregnancy experience for mother and baby.




















![Grand multiparity hi[12915]](https://cdn.slidesharecdn.com/ss_thumbnails/grandmultiparityhi12915-210509123619-thumbnail.jpg?width=640&height=640&fit=bounds)



































































