ANTENATAL CARE (DEFINITION)
Systematic supervision involving both examination and advice to women
during pregnancy
It is a coordinated approach to provide medical care and psychological
support
Should ideally begin before pregnancy and continue till delivery
3.
OBJECTIVE:
• To ensurea normal pregnancy and to deliver safely a healthy, live baby
from a healthy mother
GOALS:
• To identify high risk cases
4.
HIGH RISK FACTORSIN PREGNANCY
CATEGORY CONDITIONS
PRE EXISTING MEDICAL
CONDITIONS
• Hypertension
• Diabetes mellitus
• Heart diseases
• Respiratory diseases
• Chronic kidney diseases
• Autoimmune diseases
• Thyroid diseases
• Obesity
• History of deep vein thrombosis
• HIV positive status
• PCOS
5.
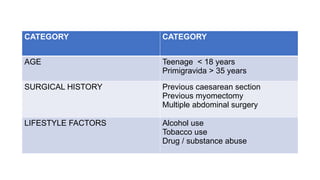
CATEGORY CATEGORY
AGE Teenage< 18 years
Primigravida > 35 years
SURGICAL HISTORY Previous caesarean section
Previous myomectomy
Multiple abdominal surgery
LIFESTYLE FACTORS Alcohol use
Tobacco use
Drug / substance abuse
6.
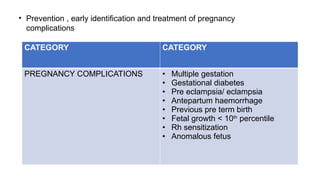
CATEGORY CATEGORY
PREGNANCY COMPLICATIONS• Multiple gestation
• Gestational diabetes
• Pre eclampsia/ eclampsia
• Antepartum haemorrhage
• Previous pre term birth
• Fetal growth < 10th
percentile
• Rh sensitization
• Anomalous fetus
• Prevention , early identification and treatment of pregnancy
complications
7.
• To educatepatients about antenatal exercise, physiology of pregnancy,
labor and childbirth through mothercraft classes using demonstrations and
classes
• To discuss place, time, mode of delivery and care of newborn
• To provide adequate psychological counselling by allying her fear
• To ensure continues medical supervision and prophylaxis
• To plan contraceptive use for the future
8.
COMPONENTS:
• Assessment duringpre- conceptional period
• Assessment during 1st
and subsequent antenatal visits
• During each visit, clinical history of the patient should be carefully noted
down.
• General physical examination , obstetric examination and appropriate
investigations should also be conducted
• Advice given to women during pregnancy
9.
PRE PREGNANCY CARE
Antenatalcare should ideally begin before conception while planning
pregnancy
• General check up to confirm physical and mental fitness of the would be
parents
• Folic acid supplementation: Recommended daily dose is
CATEGORY DOSE
No previous history of neural tube defects 500 micrograms / day
History of neural tube defects 5 mg / day
10.
• Immunity torubella should be checked and immunization given to those
not immune
• Screening for thalassemia ( as incidence is relatively high in India)
• Advice regarding diet and exercise ( more important in obese and
overweight women)
• Hazards of alcohol and tobacco consumption in pregnancy should be
explained and help provided to quit smoking and alcohol consumption
• Periconceptional counselling in women with pre existing medical conditions
such as diabetes, epilepsy, asthma, chronic kidney diseases depression
and optimization of medication and medical condition
11.
DIAGNOSIS OF PREGNANCY:
•Maternal serum or urine hCG levels : Can be detected by 8 to 9 days after
ovulation
• The doubling time of serum hCG is 1.4 to 2 days
12.
CONFIRMATION OF PREGNANCY
SONOGRAPHICRECOGNITION OF PREGNANCY
• Confirm an intrauterine pregnancy
• Estimate gestational age
• Confirm cardiac activity
• Diagnosis / evaluate a multifetal gestation, including chronicity and
amnionicity
• Assess for certain fetal anomalies, such an anencephaly
• Evaluate for uterine abnormalities or pelvic mass
13.
• Evaluate forsuspected ectopic pregnancy
• Evaluate for suspected gestational trophoblastic disease
• Evaluate cause of vaginal bleeding
14.
NORMAL DURATION OFPREGNANCY
• 280 days , 40 weeks
• Calculation of EDD :
NAEGELE,S FORMULA : LMP + 9 months + 7 days
15.
TRIMESTER NUMBER OFVISITS
1ST
TRIMESTER EVERY 4 WEEKS
2ND
TRIMESTER EVERY 4 WEEKS
3RD
TRIMESTER EVERY 2 WEEKS TILL 36 WEEKS
WEEKLY FROM 36 WEEKS TILL
DELIVERY
ANTENATAL VISITS IN AN UNCOMPLICATED SINGLETON
PREGNANCY
Total number of visits : 11 to 15
According to WHO , there should be a minimum of 1 visit in 1st
trimester, 2
visits in 2nd
trimester and 5 visits in 3rd
trimester
The 1st
visit tothe hospital : BOOKING VISIT
Ideally before 10 weeks of pregnancy
It consists of :
• History taking
• Booking examination
• Investigations at booking
OBSTETRIC HISTORY
• Durationof marriage , consanguinity
• Details of every previous pregnancy should be noted under the following
headings:
DETAILS OF DELIVERY
Duration of pregnancy
Labor : spontaneous / induced
Duration of labor
Mode of delivery : vaginal / caesarean
If operative delivery : indication
Live born / still birth
Birth weight and sex
Breastfeeding history
Present health of child
Antepartum / intrapartum/ postpartum complications
PAST HISTORY:
• Medicalhistory : History of hypertension, diabetes mellitus, thyroid
disorders, cardiac disorders, asthma , epilepsy , tuberculosis
• Past history of surgical procedures
• Allergies to food or drugs
• History of blood transfusion
• And medications that she is using chronically and whether continues in
pregnancy
PERSONAL HISTORY:
• Diet
•Appetite
• Bowel and bladder
• Smoking and alcohol intake
• Contraceptive practice prior to pregnancy
25.
HISTORY OF PRESENTPREGNANCY:
• Excessive nausea, vomiting
• Fever
• Viral infections
• Drug intake
• Exposure to teratogens
• Irradiation
• When was urine pregnancy test done to confirm pregnancy
• Conception: spontaneous / any drugs used for induction/ ART
• USG confirmation of pregnancy
26.
BOOKING EXAMINATION
GENERAL PHYSICALEXAMINATION:
• HEIGHT : A short stature : 142 cms or 4 feet 8 inches may be associated
with small pelvis
• Maternal weight
• Body mass index ( BMI) : Weight ( kgs)
Height ( meters) 2
• BREASTS:
Pregnancy changesand other abnormalities
Nipple : Flat, inverted
Any breast lump , discharge
• CARDIOVASCULAR SYSTEM:
• RESPIRATORY SYSTEM
• ABDOMINAL EXAMINATION
• PAP smear maybe taken , if she is due
29.
INVESTIGATIONS AT BOOKING
•Complete hemogram
• Blood grouping and Rh typing ( Husbands blood group and ICT if
husbands blood group is Rh positive )
• HIV , Hepatitis B , C and VDRL
• RBS
• Serum TSH
• Urine test : Protein , sugar and routine and microscopy
30.
SUBSEQUENT VISITS
• Bloodpressure : It is recorded in every visit
• Weight
• Urine analysis for protein: for protein and sugar
• Abdominal examination : done on an empty bladder with patient in dorsal
position and knees slightly flexed
• Look for scars, linea nigra and stria gravidarum, dilated veins, sinuses
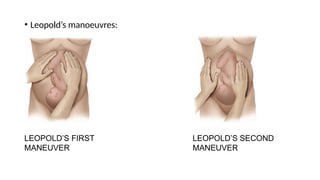
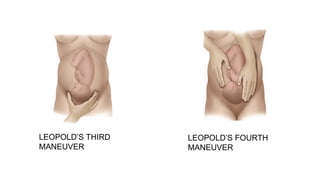
• On palpation: Fundal height, symphysio – fundal height, obstetric grips
and adequacy of amniotic fluid
• Auscultation: Fetal heart rate and its location
• ACCORDING TOFOGSI
1ST
VISIT
Ideally prior to 12 weeks
• Identify women who may need additional care and plan pattern of care for
the pregnancy.
• Start folic acid prophylaxis if not started already.
• Check blood group and Rh status.
• Offer screening for anemia, GDM -DIPSI, pre-eclampsia, hepatitis B virus,
HIV, thyroid status, rubella susceptibility, and syphilis
• Offer screening for asymptomatic bacteriuria
34.
ROUTINE ANTENATAL ANTID PROPHYLAXIS IN RHD
NEGATIVE PREGNANCY
• Repeat ICT a 28 weeks in all women with RH negative pregnancy
and offer prophylactic anti d to non immunized women
• Routine anti D prophylaxis :
Single dose of 1500 IU or 300mcg Anti D at 28 weeks
• Further followed by 1 dose of Anti D within 72 hours of delivery of a
Rh positive child
35.
TETANUS IMMUNIZATION
• Allwomen should receive 2 injections of tetanus toxoid during pregnancy
for prevention of neonatal tetanus
• Tdap ( tetanus , diphtheria, Pertussis )
It is recommended at 27 to 36 weeks of gestation
SUBSEQUENT VISITS ACCORDINGTO FOGSI
16–20 Weeks
• Immunization TT/Td/Tdap
• Measure blood pressure and test for proteinuria
• At 18–20 weeks, an ultrasound scan should be performed for
the detection of structural anomalies.
If placenta is found to extend across the internal cervical os at
this time, another scan in third trimester should be offered
38.
24–28 Weeks
• Measuresymphysio -fundal height
• Enquire about fetal movements
• Measure blood pressure and test urine for proteinuria
• Immunization Td/TT 2nd dose/Tdap
• Offer screening for GDM if negative in first visit or missed in first visit
• Offer a second screening for anemia
• Offer anti-D to Rh negative women ( 1500 IU )
39.
30–36 Weeks
• Measureblood pressure and test urine for proteinuria
• Measure symphysio-fundal height
• Enquire about fetal movements
• Check fetal heart
• USG if feasible for fetal growth, placenta, and well-being
40.
36–40 Weeks
• Measureblood pressure and test urine for proteinuria
• Measure Haemoglobin
• Enquire about fetal movements
• Measure symphysio–fundal height
• Check position of baby and fetal heart
• Review ultrasound scans report
41.
After 40 Weeks
Forwomen who have not delivered by 41
weeks:
• Closer antepartum vigilance
• Measure blood pressure and test urine for proteinuria
• Enquire about fetal movements
• Measure symphysis-fundal height
• Check position of baby
• Consider induction if inducible and favourable cervix
42.
SCREENING FOR DOWN’SSYNDROME:
• First trimester combined screening : 11 weeks to 13 weeks 6 days
NT scan and double marker ( beta hCG and pregnancy associated plasma
protein A ( PAPPA)
• Triple or quadruple test : 15 to 19 weeks
Alpha feto protein
Beta hCG
Estriol
Inhibin A
CALORIES
• Eating fortwo’ is a myth and results only in excessive weight gain
during pregnancy.
• The daily caloric intake should be increased by about 300 kcal, the
normal daily requirements in pregnancy do not generally exceed 2500
kcal.
• The weightgain should not exceed 2½ kg in a month or 0.9 kg in a
week.
• Excessive weight gain, in women has been shown to be associated
with increased incidence of gestational hypertension ,Pre-
eclampsia ,gestational diabetes ,macrosomia ,caesarean delivery.
• Low maternal weight gain (<6 kg) in underweight women may be
associated with IUGR.
47.
•PROTEINS
• During thesecond half of pregnancy, approximately 1000 g of protein
are deposited, amounting to 5 to 6 g/d . To accomplish this, protein
intake that approximates 1 g/kg/d is recommended.
• Meat, poultry, seafood, beans, peas, eggs, processed soy products,
nuts, and seeds all contain protein.
48.
IRON SUPPLEMENTS INPREGNANCY
• Liver, green vegetables and meat are natural sources of iron.
• Tea and coffee should be avoided immediately after meals as it interferes
with iron absorption from the gut.
• WHO recommends daily oral iron 30–60 mg of elemental iron. The
equivalent of 60 mg of elemental iron is 300 mg of ferrous sulfate
heptahydrate, 180 mg of ferrous fumarate, or 500 mg of ferrous gluconate
49.
FOLIC ACID SUPPLEMENTSIN PREGNANCY
• WHO recommends daily folic acid supplementation with and 400 µg (0.4 mg)
of folic acid in pregnant women to prevent maternal anaemia.
• Periconceptional folic acid has been shown to reduce the risk of NTDs and
other birth defects like cleft lip and congenital heart disease and it should be
started preferably before pregnancy and continued through the first
trimester.
• The recommended dose of folic acid in women with-out any history of
previous NTD affected baby is400 µg/day, and 4 mg/day in women with
affected pregnancy.
50.
Doses of folicacid in special cases
• Diabetic female: prophylactic dose
• Patient on anti-epilectic drugs- before conception-400mcg/day
After conception-4mg/day
Sickle cell anemia:5g/day
Megaloblastic anemia:1g/day.
51.
IRON AND FOLICACID SUPPLEMENTS
• According to Government of India National Health Policy 2017
recommendations, all pregnant women must receive a tablet of
100mg of elemental iron and 500 µg of folic acid for at least 100 days
in pregnancy starting after first trimester, and for another 100 days
postpartum
• According to Anemia Mukt Bharat Programme: 60mg elemental
iron+500mg of folic acid(red)
• 1tab/day given for non anemic pregnant women for 180 days during
pregnancy and 180 days after pregnancy.
52.
CALCIUM IN PREGNANCY
•RDA-1000mg/day
• In populations with low dietary intake of calcium, WHO recommends 1.5–
2.0 g of oral elemental calcium supplementation daily.
• Sources: Milk, Cheese, Yoghurt,Sardines, dark green leafy vegetables.
• Adequate calcium supplementation may play a role in the prevention of
pregnancy induced hypertension as well. Salt encourages the urinary
excretion of calcium, so its intake should be minimised.
7.NAUSEA AND HEARTBURN
8.PICA AND PTYALISM
9.HEADACHE OR BACKACHE
10.VARICOSITIES AND HEMORRHOIDS
11.SLEEPING
55.
EMPLOYMENT
• The Familyand Medical Leave Act of 1993 requires that covered
employers must grant up to 12 work weeks of unpaid leave to an
employee for the birth and care.
• In the absence of complications, most women can continue to work
until labor onset.
• According to the American College of Obstetrics and Gynecologists,
risks of preterm birth are slightly to modestly increased with standing
or walking at work >3hours daily , lifting, and carrying >5kg, or
physically exerting oneself at work.
56.
EXERCISE
• In theabsence of contraindications for exercise pregnant women are
encouraged to engage in regular , moderate-intensity physical activity
for atleast 150 minutes each week.
• Examples of Safe activities are walking, running, swimming ,stationary
cycling and low impact aerobics.
• However they should refrain from activities with high risk of falling or
abdominal trauma.
57.
• As ageneral guideline, 30 minutes or more of moderate exercise a day on
most, if not all, days of the week is recommended for pregnant women.
• Exercise increases the pulse rate, but the blood pressure and temperature
remain unaffected. Being active during pregnancy also helps in reducing
backache, constipation and edema
58.
CONTRAINDICATIONS TO EXERCISE
•Significant cardiovascular or pulmonary disease: chest pain, calf pain
or swelling.
• Significant risk for preterm labor: cerclage, multifetal gestation,
significant bleeding, threatened preterm labor, ruptured membranes.
• Obstetrical complications: preeclampsia, placenta previa, anemia,
poorly controlled diabetes or epilepsy, morbid obesity.
59.
SLEEP
• A minimumof eight hours in bed at night, preferably 10.
• during the afternoon the expectant mother should be encouraged to
lie down or at least put her feet up for an hour.
SMOKING
• mean birth weight of the babies of mothers who smoke is lower and
the prematurity rate higher than in non-smokers
60.
• For thepatient who has a known tendency to abort, travel is
contraindicated during the first trimester. Women at risk of preterm
labor should also avoid travel.
• Long car journeys should be interrupted about every two hours in
order to allow a change of position and the re-establishment of
healthy circulation.
TRAVEL
61.
• Travel byair nowadays in pressurized aircraft has no risks to
pregnancy and is particularly suitable for long journeys because it
reduces the travel time.
• In the absence of obstetrical or medical complications, the American
College of Obstetricians and Gynecologists (2018a) has concluded that
pregnant women can safely fly up to 36 weeks' gestation
62.
CAFFEINE
• Heavy Intakeof coffee each day-approximately five cups or 500 mg of
caffeine-slightly raises the miscarriage risk.
• CARE Study Group (2008), however, evaluated 2635 low-risk
pregnancies and reported a 1.4-fold risk for fetal-growth restriction
among those whose daily caffeine consumption was > 200 mg/d
compared with those who consumed <100 mg/d
63.
COITUS
• Pregnant womenshould be informed that sexual intercourse during
pregnancy is not known to be associated with any adverse effects
unless there is a history of bleeding in the pregnancy or a low-lying
placenta.
64.
NAUSEA AND VOMITING
•CAUSE: Hcg+estrogen+progesterone.
• Peaks at 10 weeks of pregnancy due to hcg peak.
• Subsides by 16 weeks of pregnancy.
• TREATMENT: small frequent meals, avoid spicy meals and fatty meals.
DOC: PYRIDOXINE(10MG) + DOXYLAMINE(10MG)
METOCLOPRAMIDE/PROMETHAZINE
ONDENSETRON
65.
PICA AND PTYALISM
•Craving for strange foods is termed as Pica.
• Ice-pagophagia
• Starch-amylophagia
• Clay-geophagia.
• Cravings usually abate once deficiency correction.
• Women during pregnancy are occasionally distressed by profuse
salivation-Ptyalism usually by the ingestion of starch.
66.
BACKACHE
CAUSES-laxity of joints(dueto estrogen,relaxin)
Weight gain
Faulty posture
Hyperlordosis
TREATMENT-
Correction of posture
Elevate lower limb while resting
Use of hard bed
Back massage
Analgesics
67.
VARICOSITIES
• Venous legvaricosities have a congenital predisposition.
PATHOPHYSIOLOGY
• Femoral venous pressures in the supine gravida rise from 8 mm Hg in early
pregnancy to 24 mm Hg at term. Thus, leg varicosities typically worsen as
pregnancy advances, especially with prolonged standing.
• Decreased vascular resistance.
• Increased blood volume.
• Progesterone-smooth muscle relaxant
68.
TREATMENT
• AVOID STANDINGFOR LONG HOURS
• LEG ELEVATION WHILE RESTING
• USE COMPRESSION STOCKINGS
• LIE IN LEFT LATERAL POSITION.
• NO MEDICAL OR SURGICAL DONE DURING PREGNANCY.

















































![Antenatal_Care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antenatalcare1-221127110720-810db45a-thumbnail.jpg?width=640&height=640&fit=bounds)
![Prenatal[3]](https://cdn.slidesharecdn.com/ss_thumbnails/prenatal3-120201220429-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















