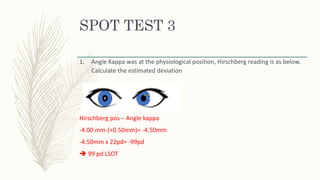
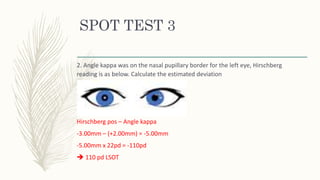
Angle kappa was on the nasal pupillary border for the left eye, indicating exotropia. The Hirschberg reading was -3.00mm.
To calculate the estimated deviation:
- Subtract the angle kappa position (+2.00mm nasal) from the Hirschberg reading (-3.00mm) giving -5.00mm
- Multiply the result (-5.00mm) by 22 (prism diopters per millimeter) giving -110 prism diopters
Therefore, the estimated deviation is 110 prism diopters of left exotropia.