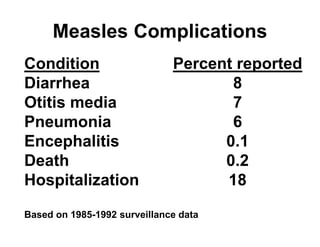
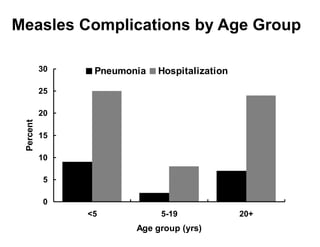
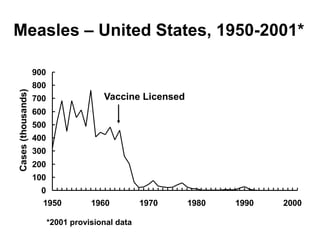
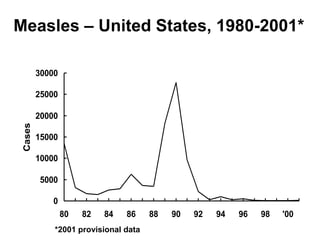
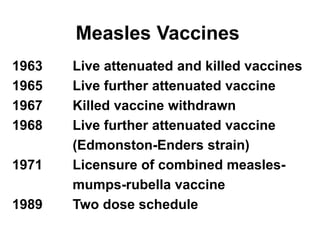
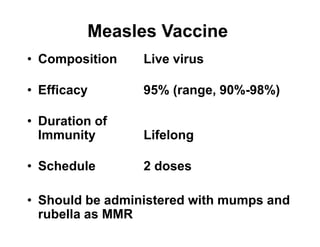
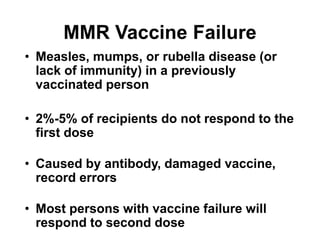
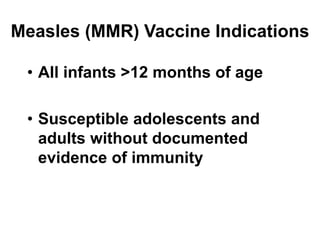
This document summarizes key information about measles and the measles vaccine. It describes measles as a highly contagious viral illness that was nearly universal before vaccination. It discusses the measles virus, clinical features of measles, epidemiology, complications, laboratory diagnosis, and vaccination recommendations including the two-dose schedule of the live attenuated MMR vaccine. The vaccine is highly effective and its safety has been demonstrated in numerous studies finding no link between MMR and autism.