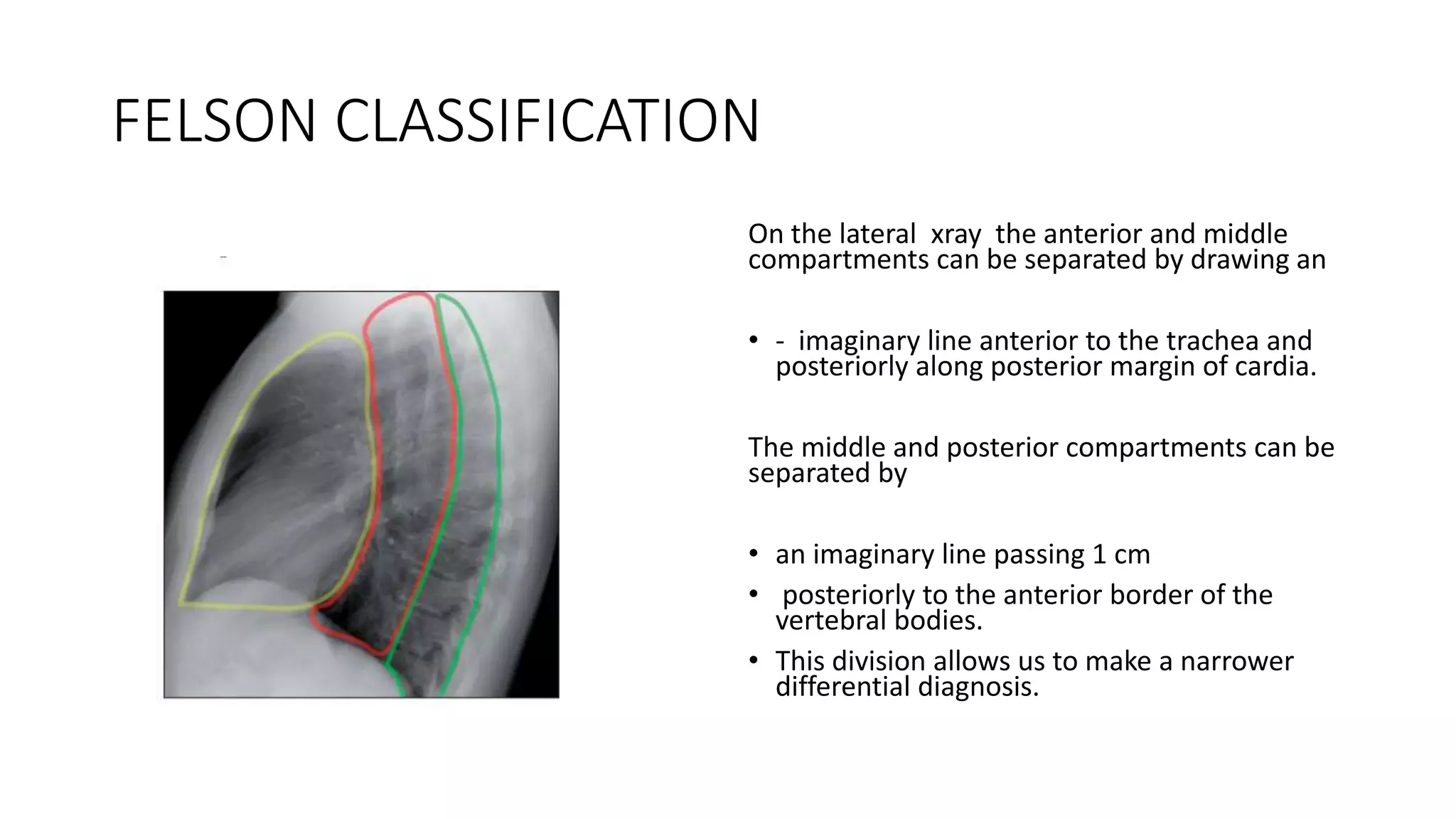
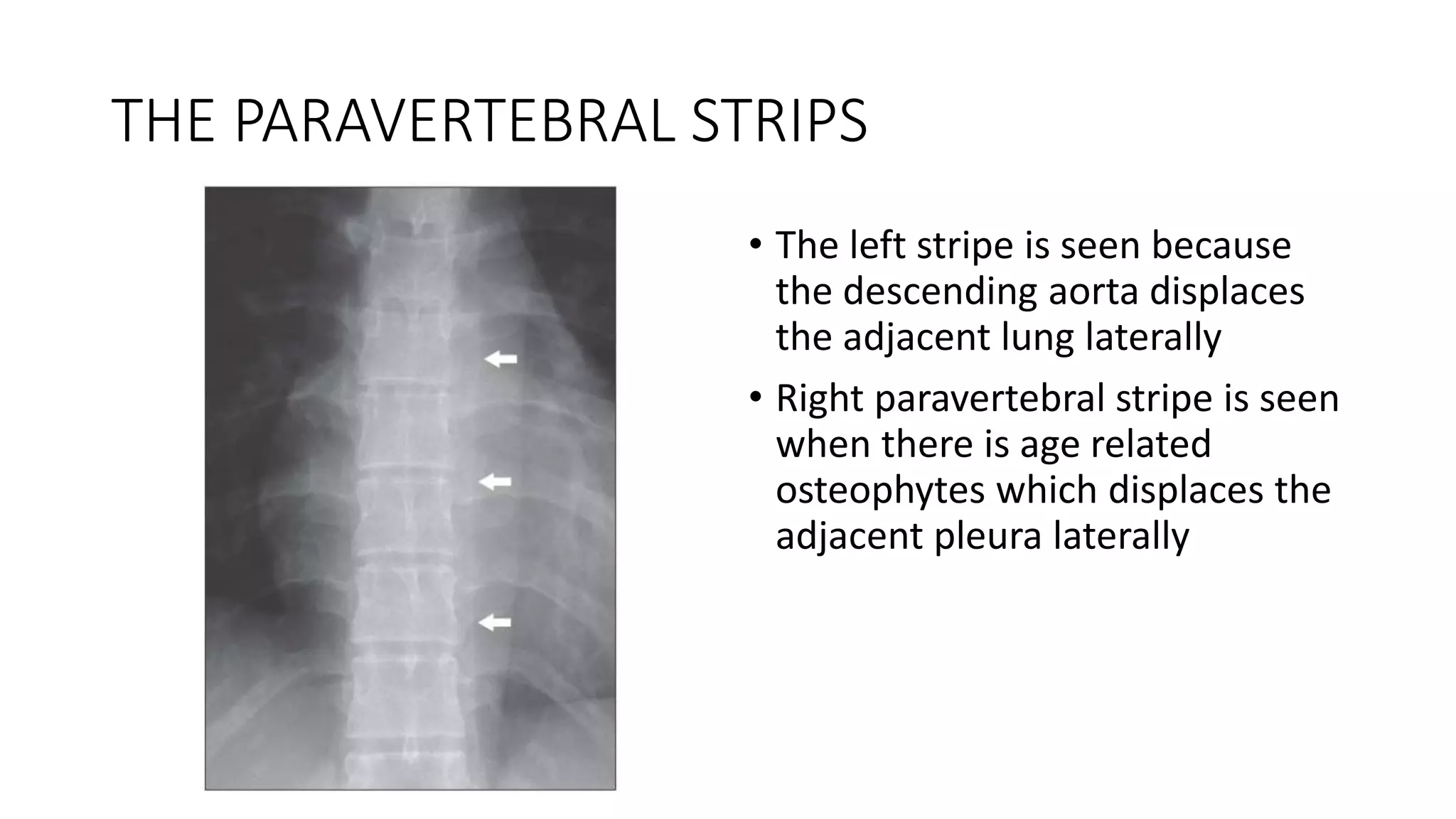
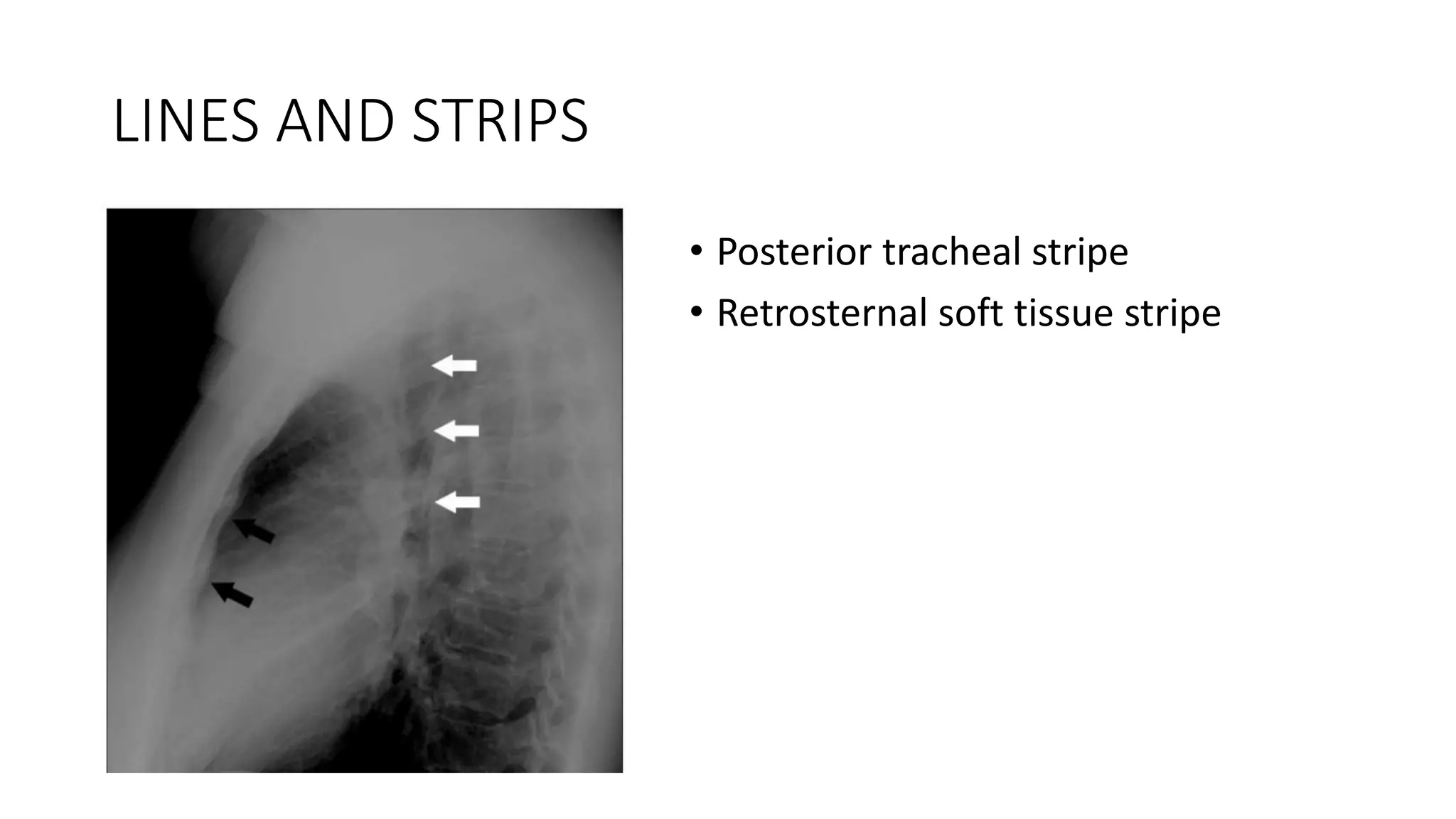
The document describes the anatomy and classification of the mediastinum. The mediastinum is located between the lungs, bounded by the thoracic inlet, diaphragm, pleurae, vertebral column and sternum. It is classified by the Sutton and Felson systems. Sutton divides it into anterior, middle and posterior compartments. Felson's classification allows for a narrower differential diagnosis by using imaginary lines to further separate the compartments on x-ray. The document also describes common fat collections and interface lines seen on frontal and lateral chest x-rays that are important for radiologists to recognize.