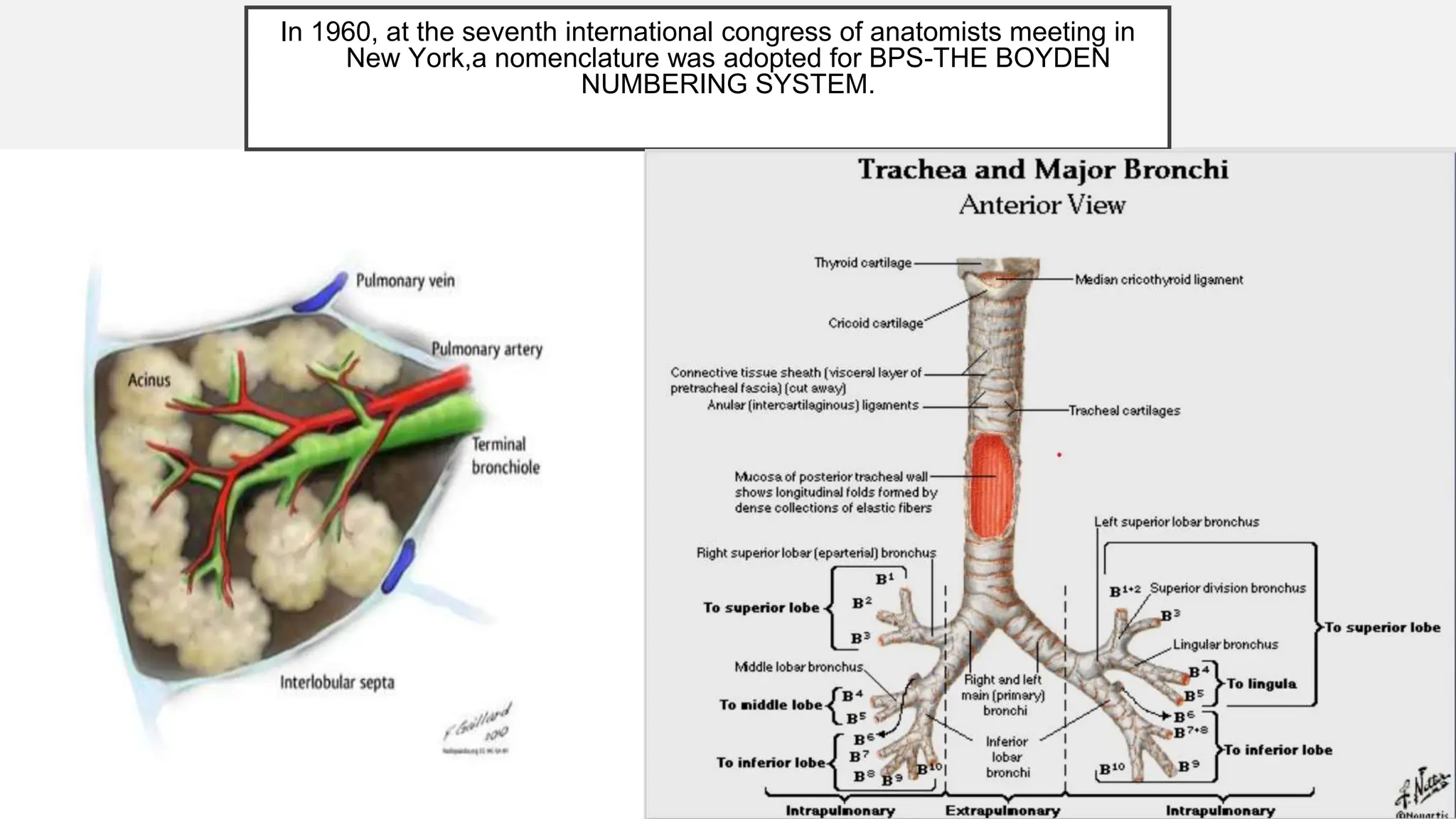
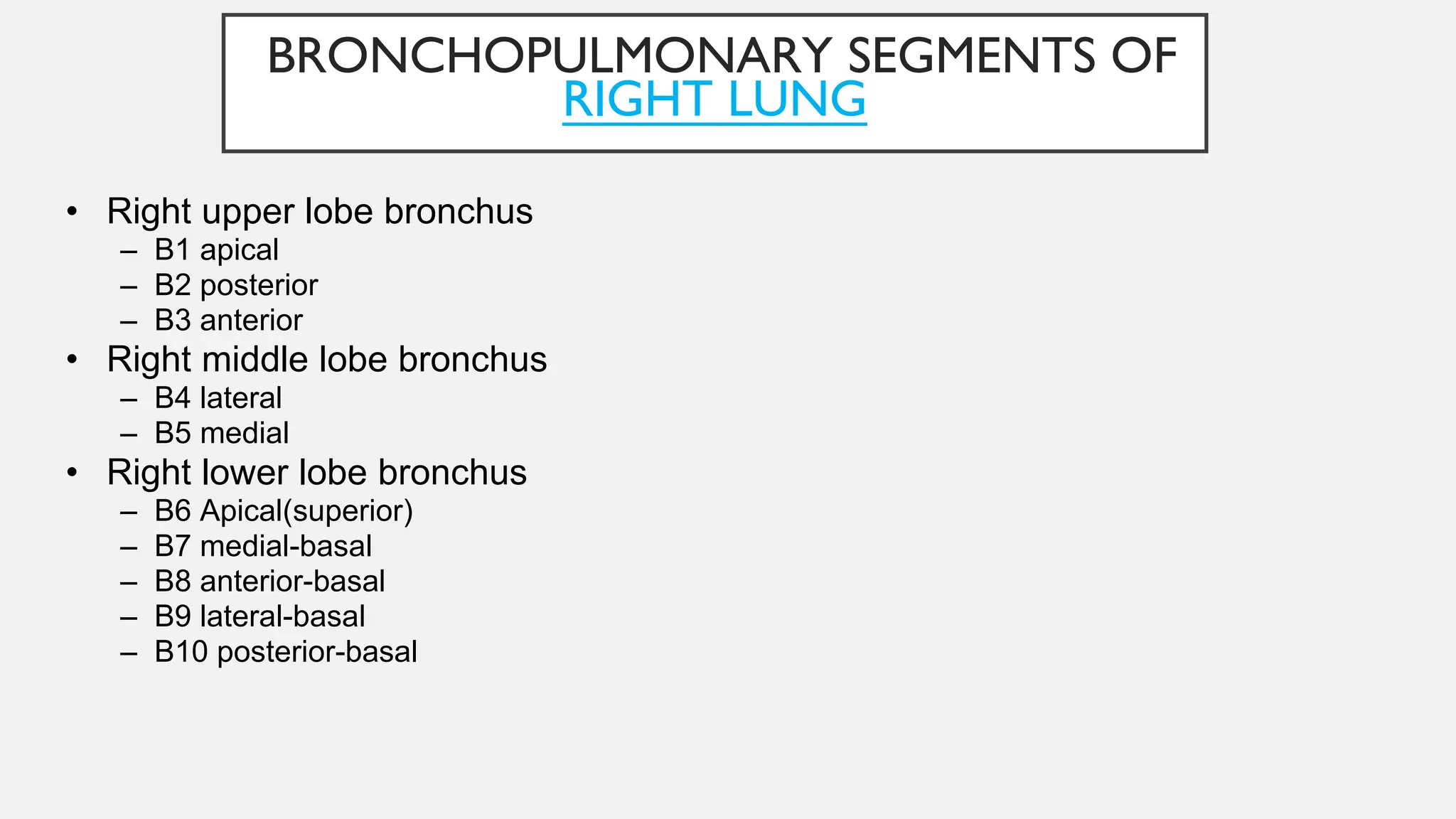
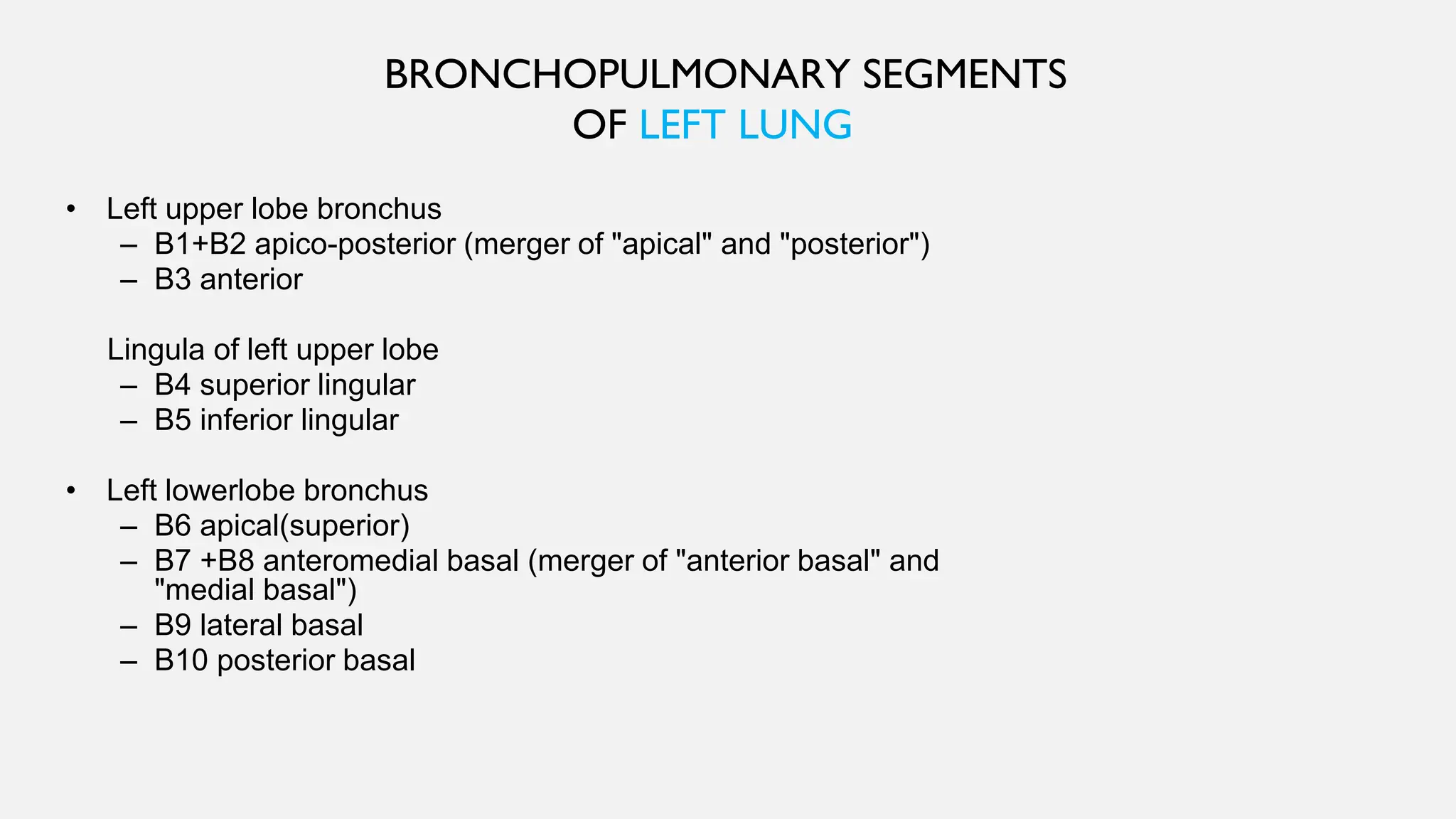
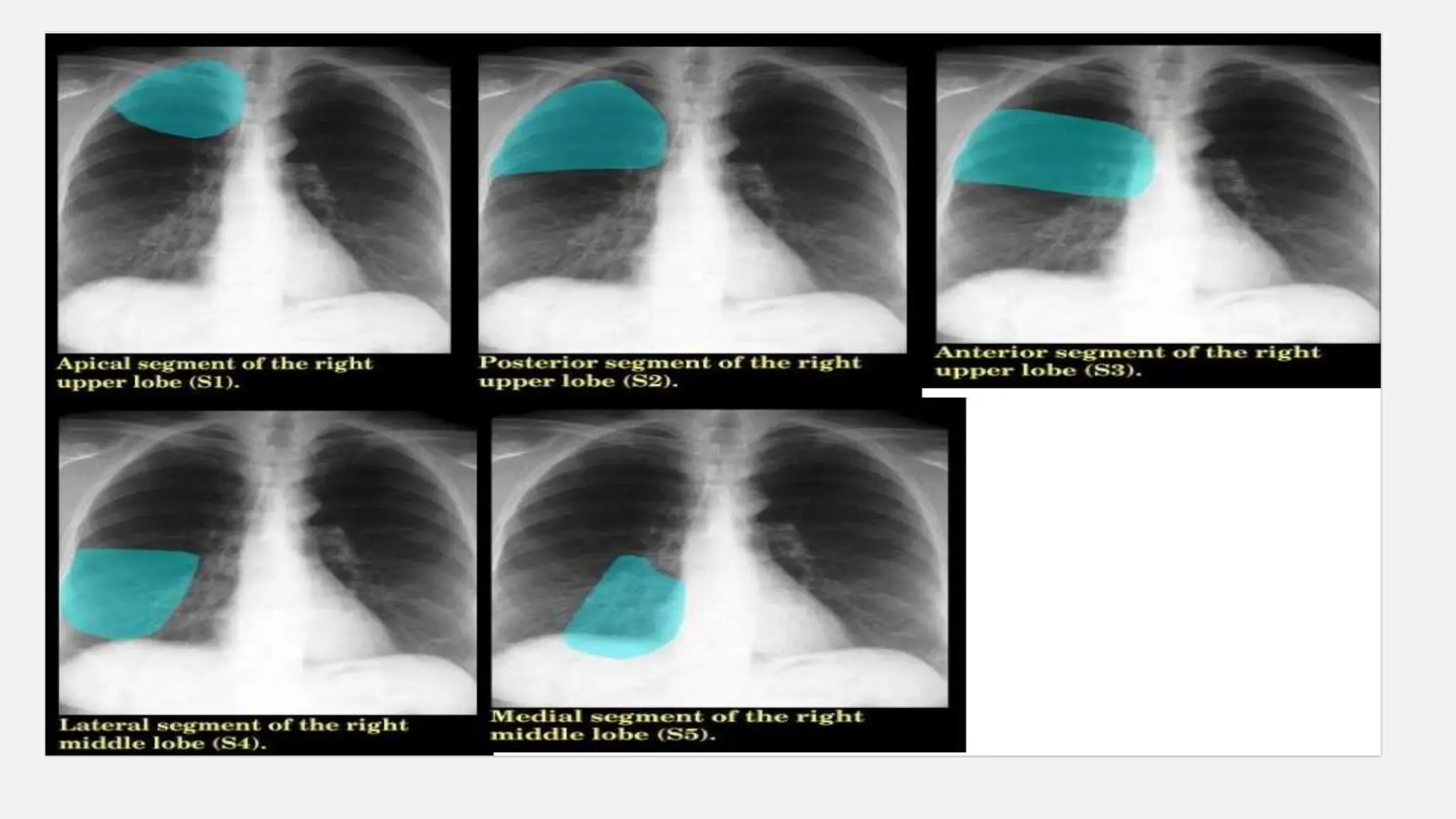
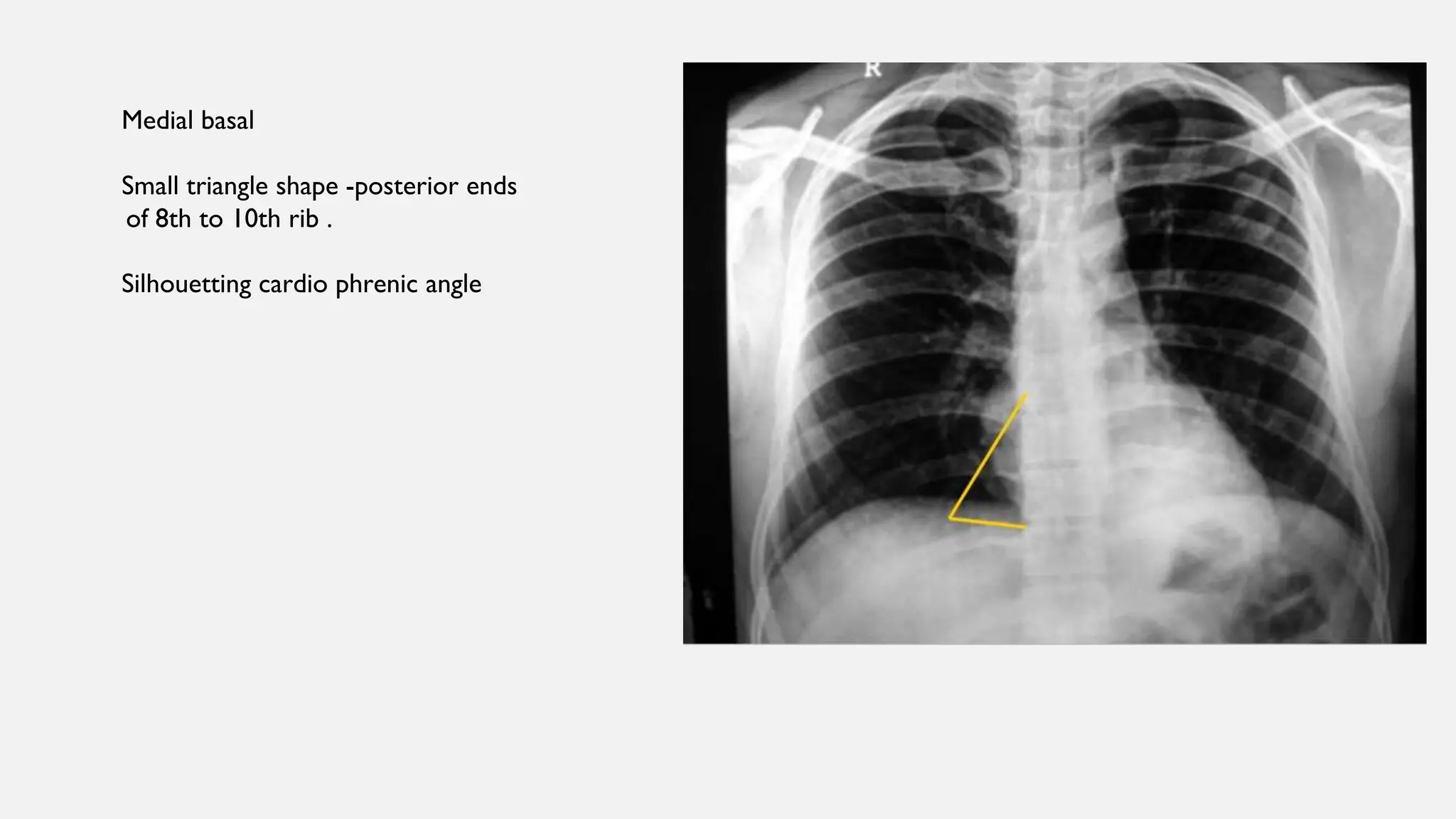
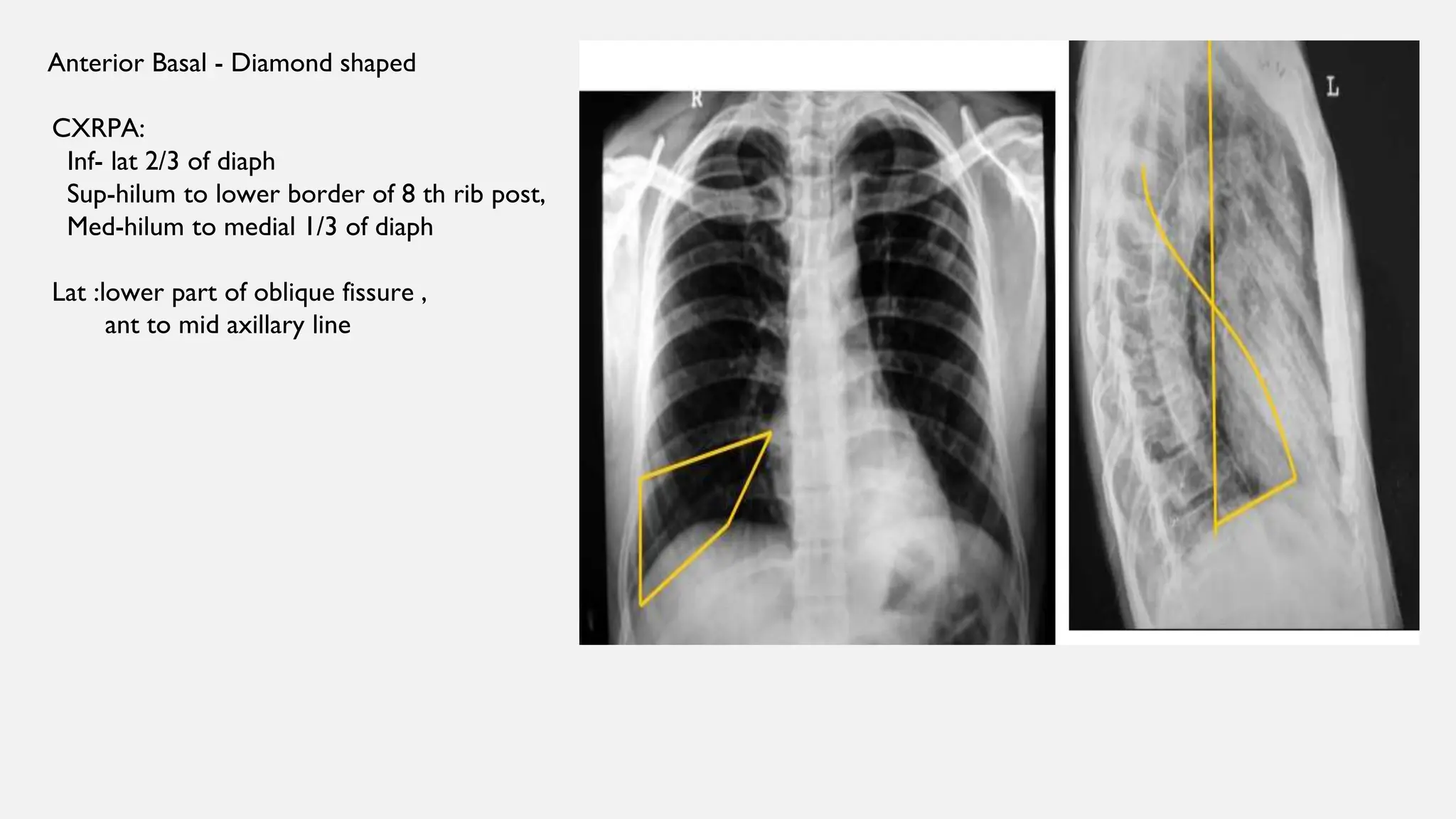
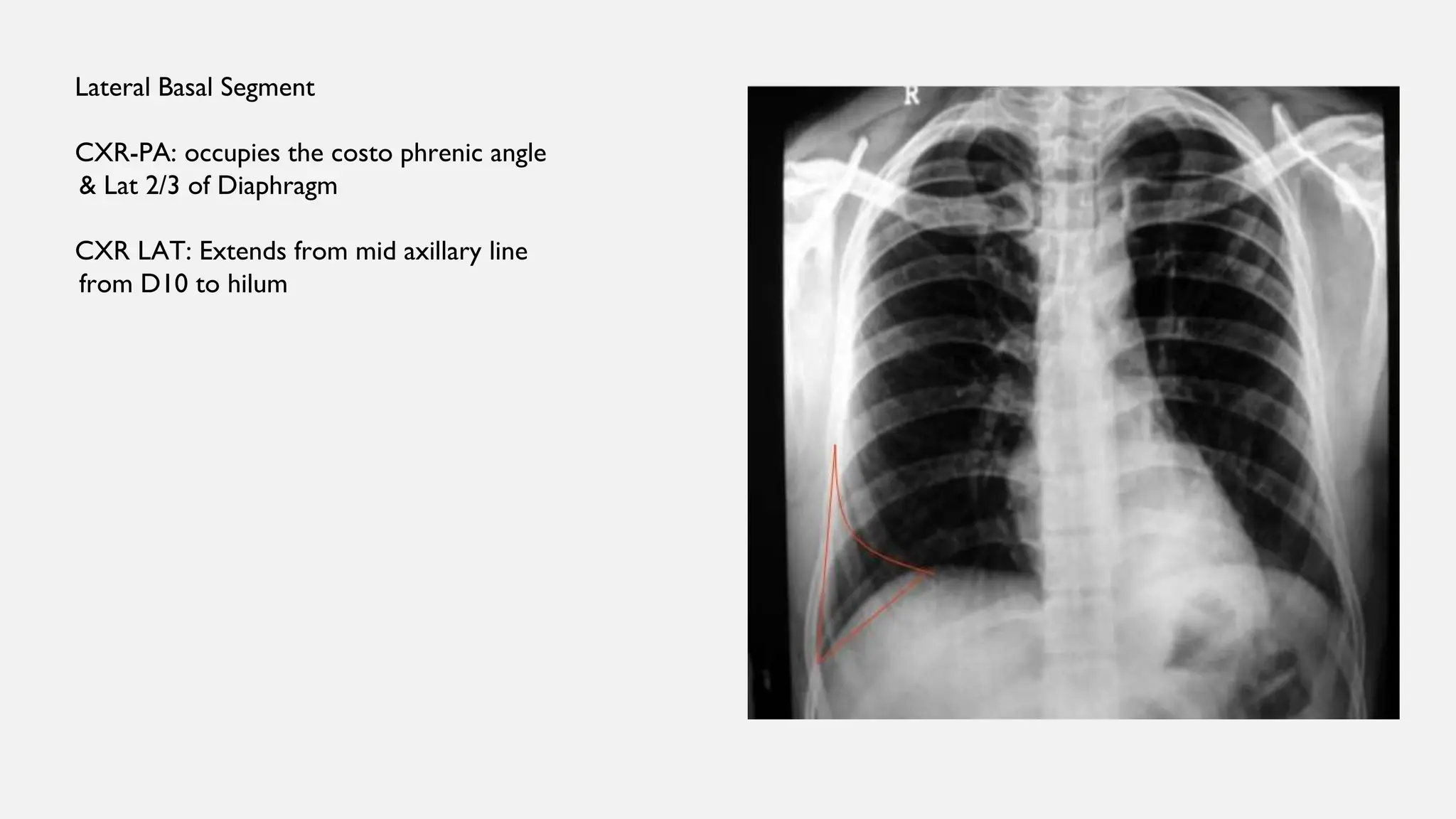
The document provides a detailed anatomical overview of the bronchopulmonary segments of the right and left lungs, outlining their respective lobar structures and segmentations. It explains the bronchial tree and the function of each segment, including distinctions in structure and clinical significance, particularly in relation to imaging techniques such as chest X-rays and CT scans. The document also discusses surgical resection principles and indications for treating conditions like tuberculosis, cancer, and bronchiectasis.