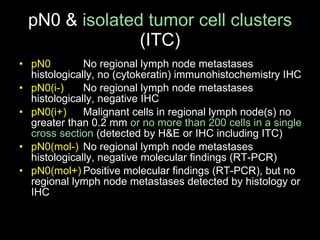
![BC is more common in…(risk factors ) Sex Elderly women (average age at diagnosis >60 y ) A subset of premenopausal (younger) women with strong family history of BC (and/or ovarian cancer) [ BRCA1, BRCA2] Western women as compared to Asian women Obese postmenopausal women With inactivity Women with long reproductive life (early menarche and late menopause) Nulliparous women as com p ared to multiparous Women having their first child after the age of 30 Therapeutic irradiation of the breast at a young age Following some pathological findings: ADH, ALH ; ipsilateral or contralateral breast cancer .](https://image.slidesharecdn.com/1-1breastca-epidemiologyandpathologyshort-110527091506-phpapp02/85/BALKAN-MCO-2011-G-Cserni-Epidemiology-and-pathology-6-320.jpg)

![TNM7: Primary tumor: (c)T & pT T & pT T X : Cannot be assessed (to be minimized) ( including R2 ) T0: No tumor Tis: in situ carcinoma (DCIS) (LCIS) (Paget) – only „pure” Paget’s disease (TNM7) (only Paget’s disease without tumor – TNM6 ) T1 (up to and inclusive of 2 0 m m); pT1mi (pT1mic – TNM6 ): 1 mm maximum size invasive focus (foci) „ … rare cases … in the absence of noninvasive disease . ” pT1a: ≤ 5 mm invasive carcinoma ( TNM7 UICC gives definition in cm ) pT1b: > 5 mm and ≤ 10 mm invasive carcinoma pT1c: >10 mm and ≤ 20 mm invasive carcinoma T2: >2 0 m m and ≤ 5 0 m m invasive carcinoma T3: >5 0 m m invasive carcinoma T4: direct extension to chest wall (pectoral muscles are not part of it) (T4a) or skin (T4b) [skin edema, ulceration, cutaneous satellite nodules] or both (T4c) or inflammatory carcinoma (at least one 3rd of the skin to be involved) (T4d)](https://image.slidesharecdn.com/1-1breastca-epidemiologyandpathologyshort-110527091506-phpapp02/85/BALKAN-MCO-2011-G-Cserni-Epidemiology-and-pathology-28-320.jpg)
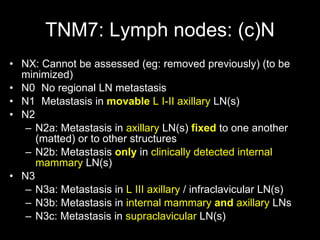
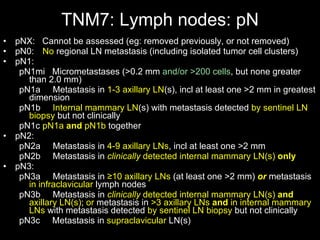

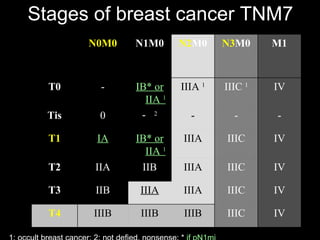
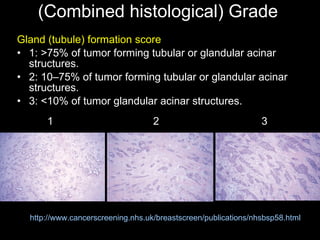
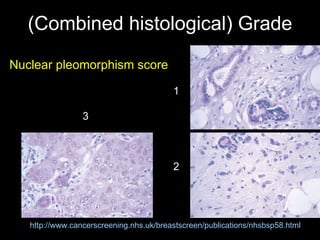
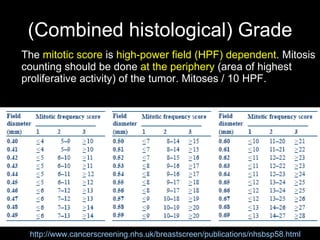
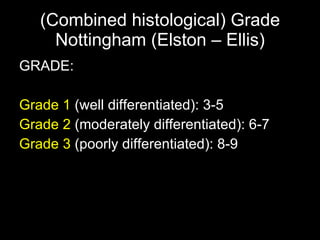
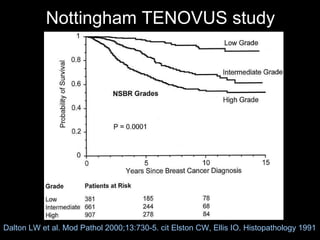
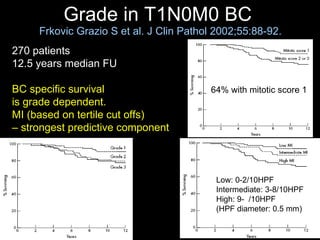

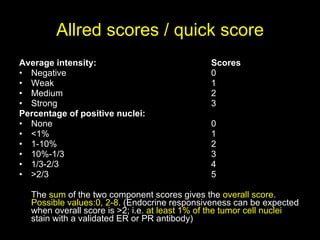
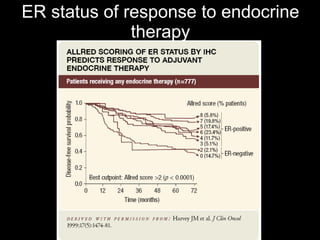
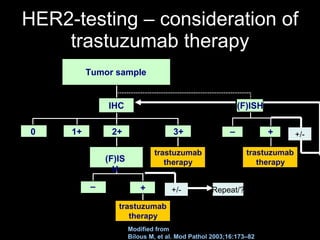

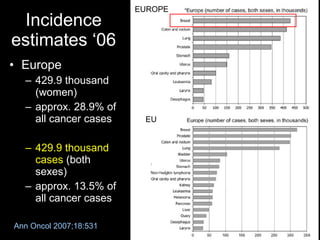
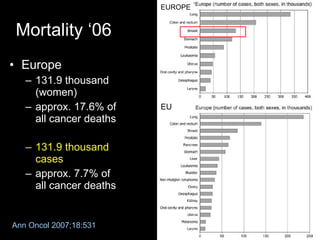
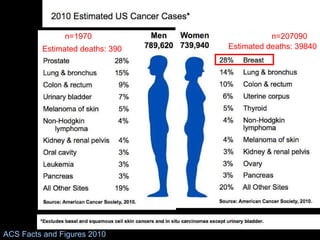
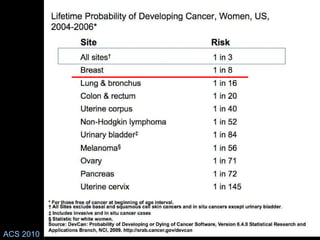
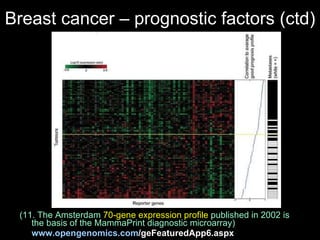
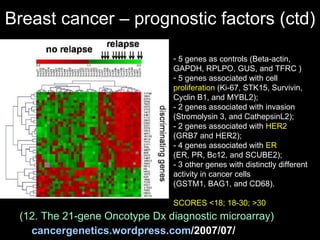
This document summarizes key information about breast cancer epidemiology and pathology. It states that in 2006 there were approximately 429,900 new breast cancer cases and 131,900 deaths from breast cancer in Europe. Risk factors for breast cancer include being female, older age, family history, obesity, lack of physical activity, reproductive factors, and prior radiation exposure. Prognostic factors associated with worse outcomes include larger tumor size, lymph node involvement, higher histologic grade, lymphovascular invasion, and hormone receptor-negative or HER2-positive status. The TNM staging system is described.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








