This document discusses breast cancer, including its definition, risk factors, types, staging, diagnosis, and treatment. Breast cancer begins in the breast tissue and may start in the ducts or lobes. It is characterized by uncontrolled cell growth. Some key points:
- Invasive ductal carcinoma is the most common type, accounting for around 80% of cases.
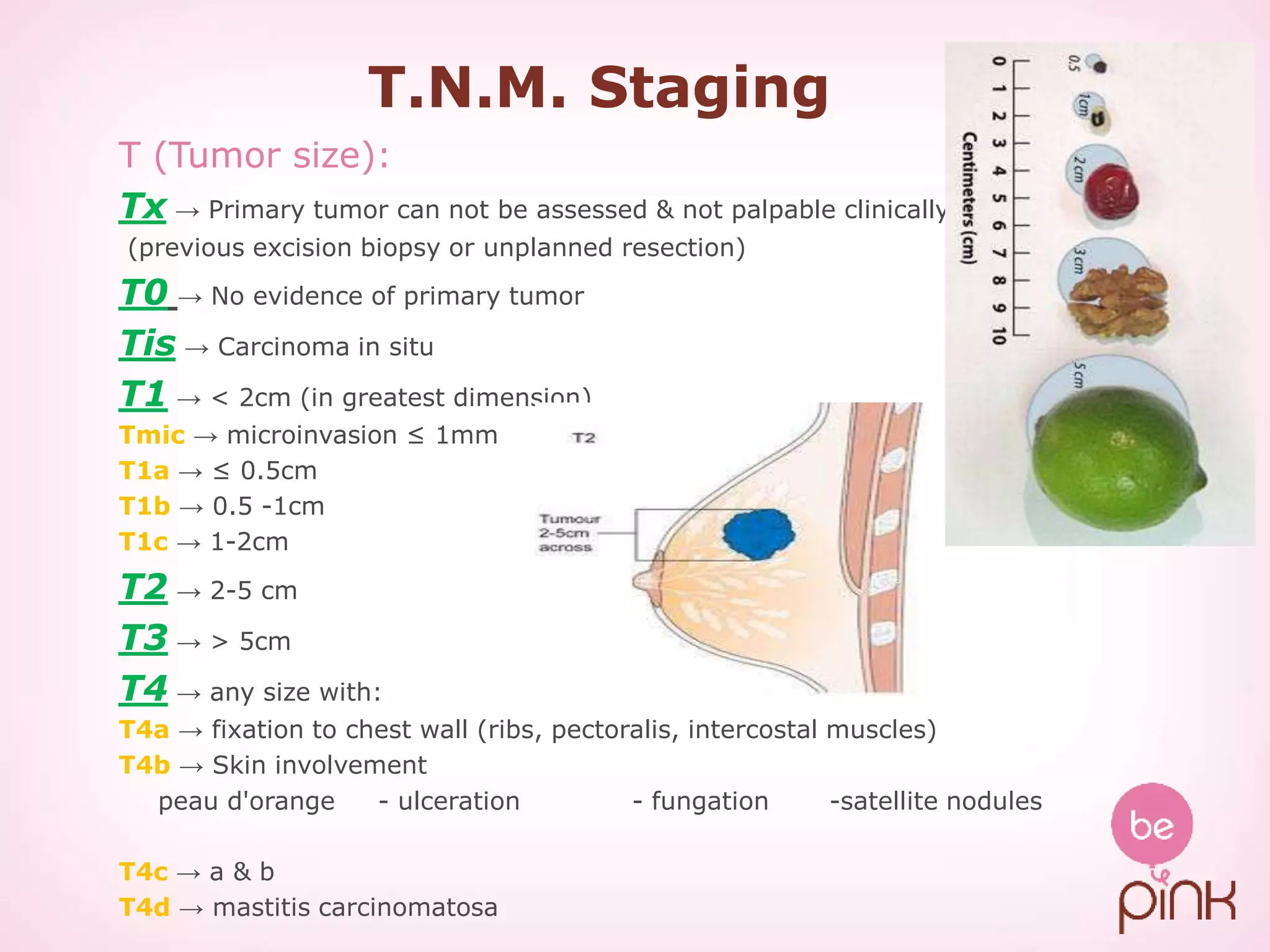
- Staging uses the TNM system to classify tumors by size (T), lymph node involvement (N), and metastasis (M).
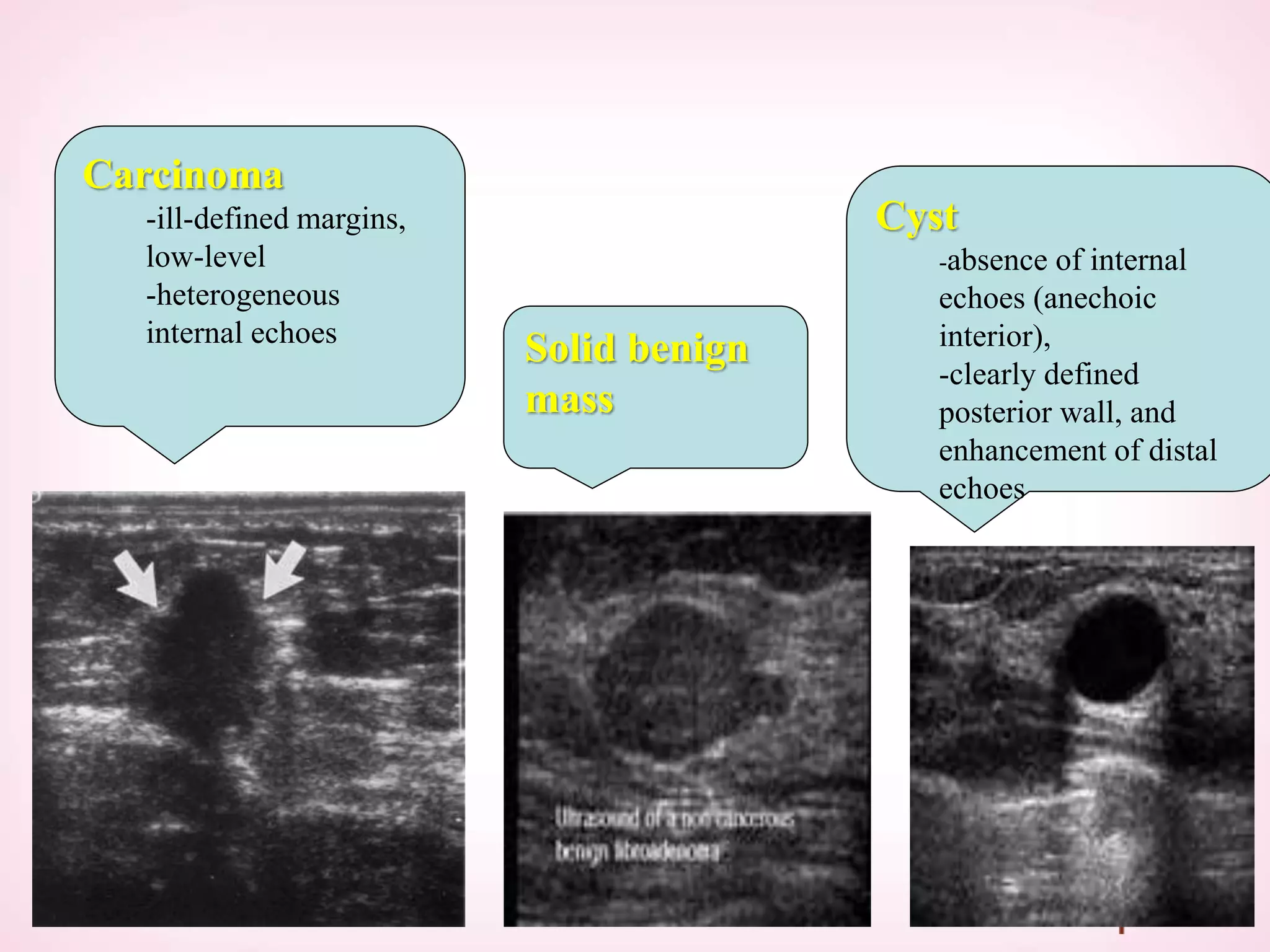
- Diagnosis involves clinical examination, imaging like mammography, and biopsy.
- Treatment depends on stage but commonly involves surgery, radiation, chemotherapy, hormone therapy, or a combination.