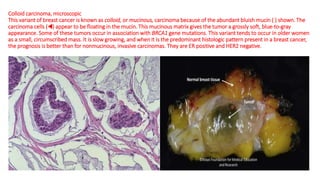
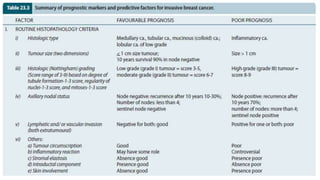
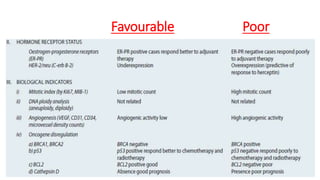
This document provides information on types and management of breast cancer. It discusses non-invasive and invasive breast carcinomas, including specific types like colloid carcinoma. Prognostic factors are described such as tumor grade and stage. Management of triple negative breast cancer is also covered, noting it is more aggressive and difficult to treat. A new vaccine study aims to prevent triple negative breast cancer.