

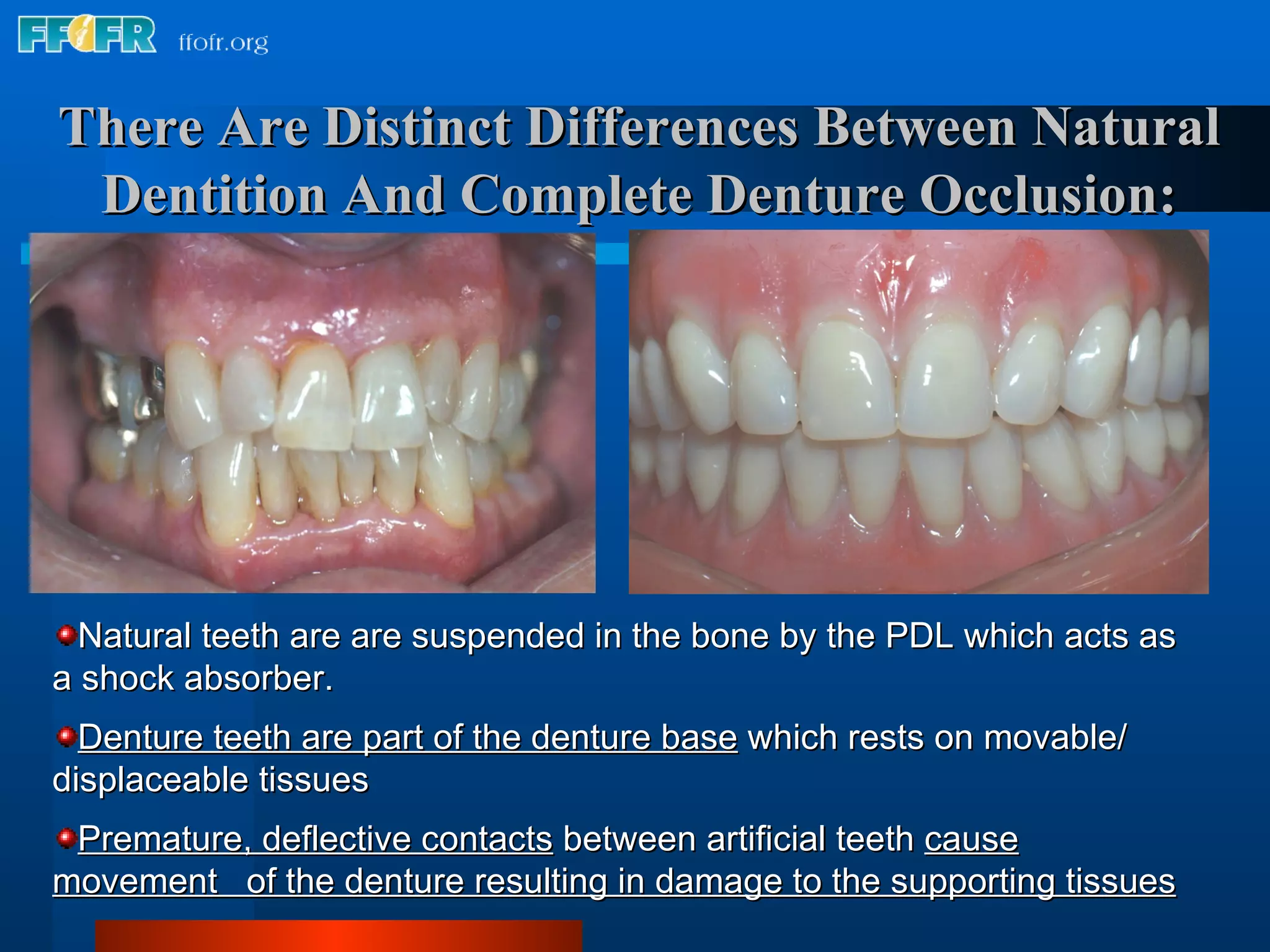

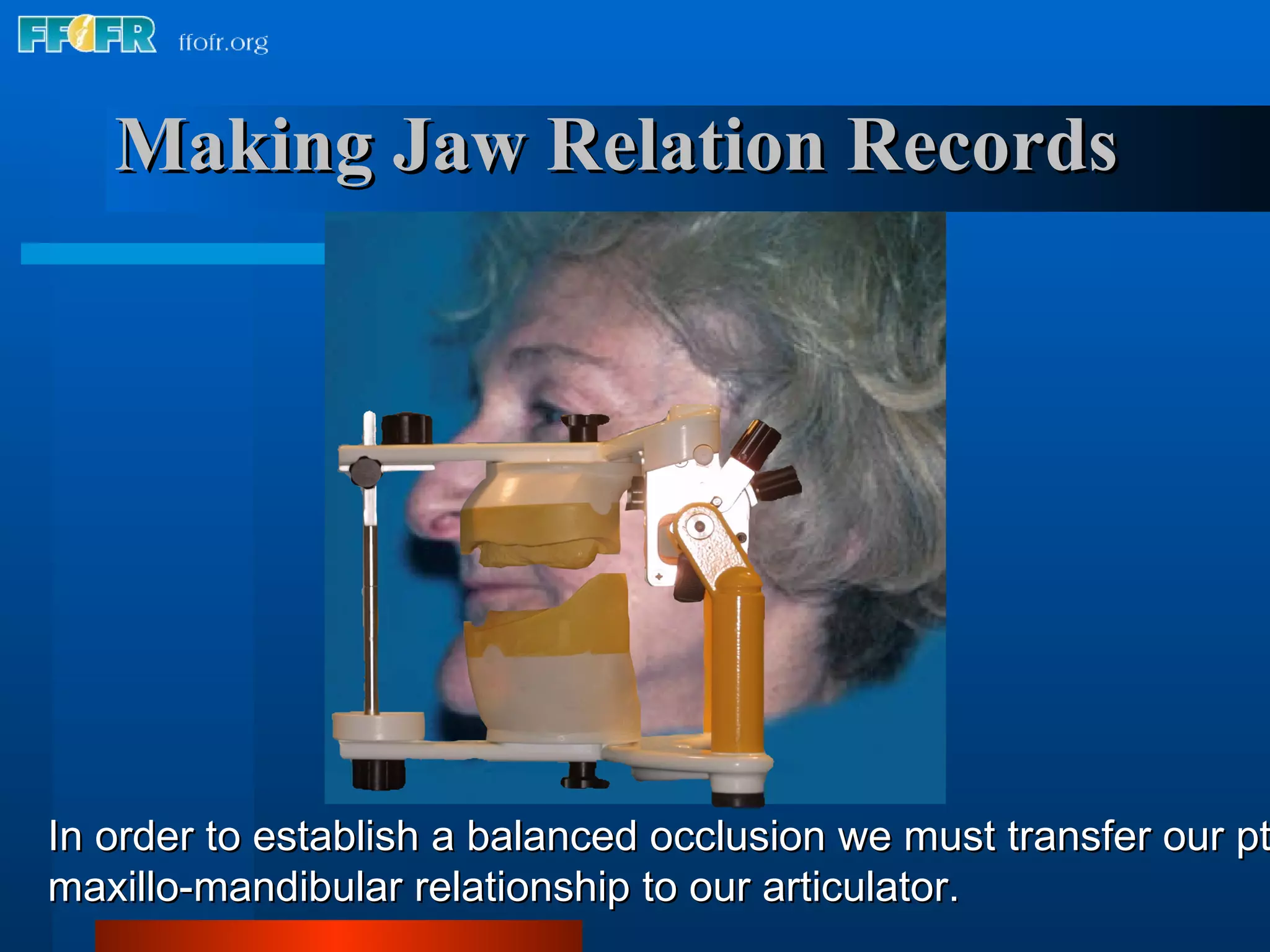

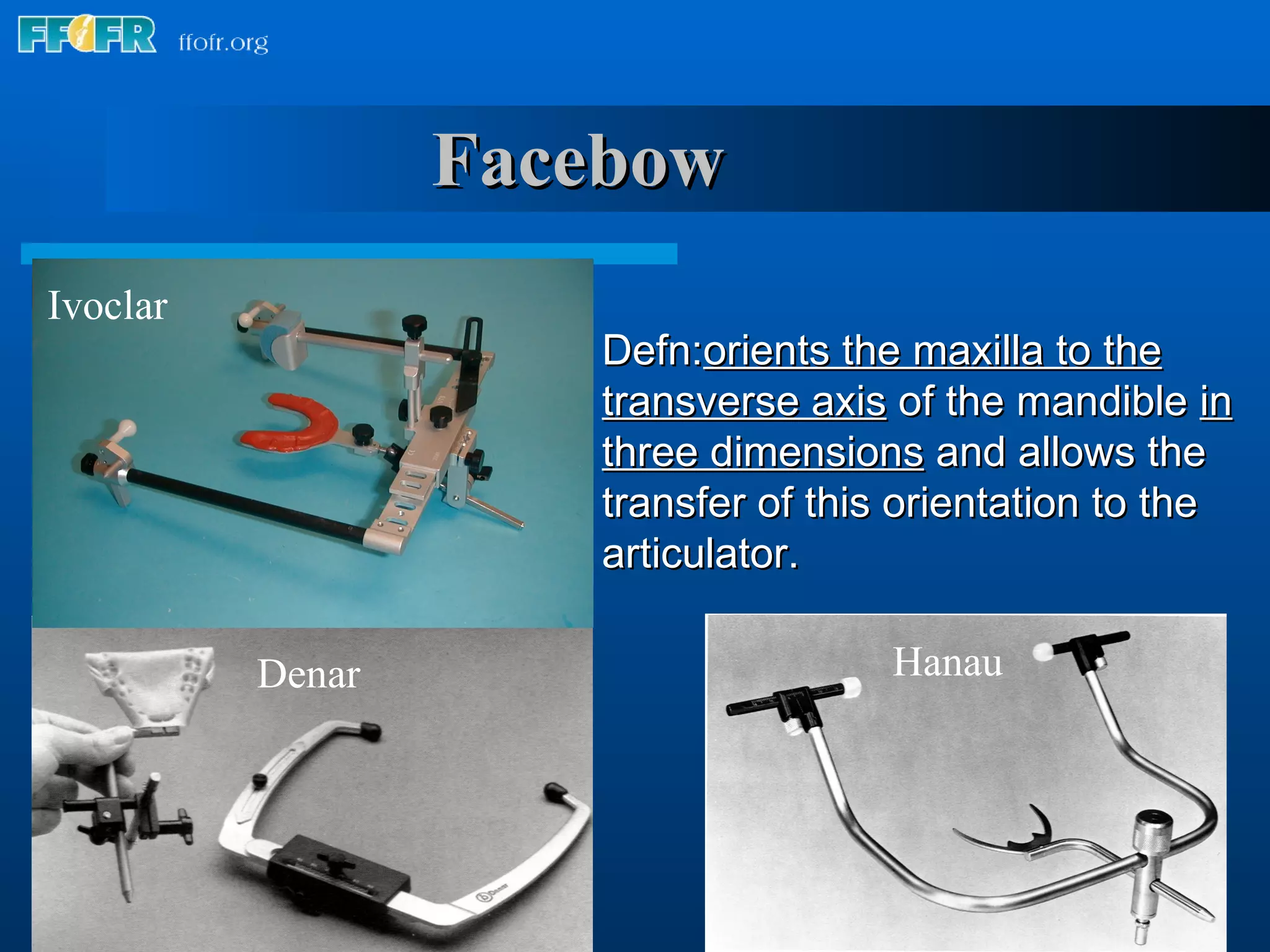


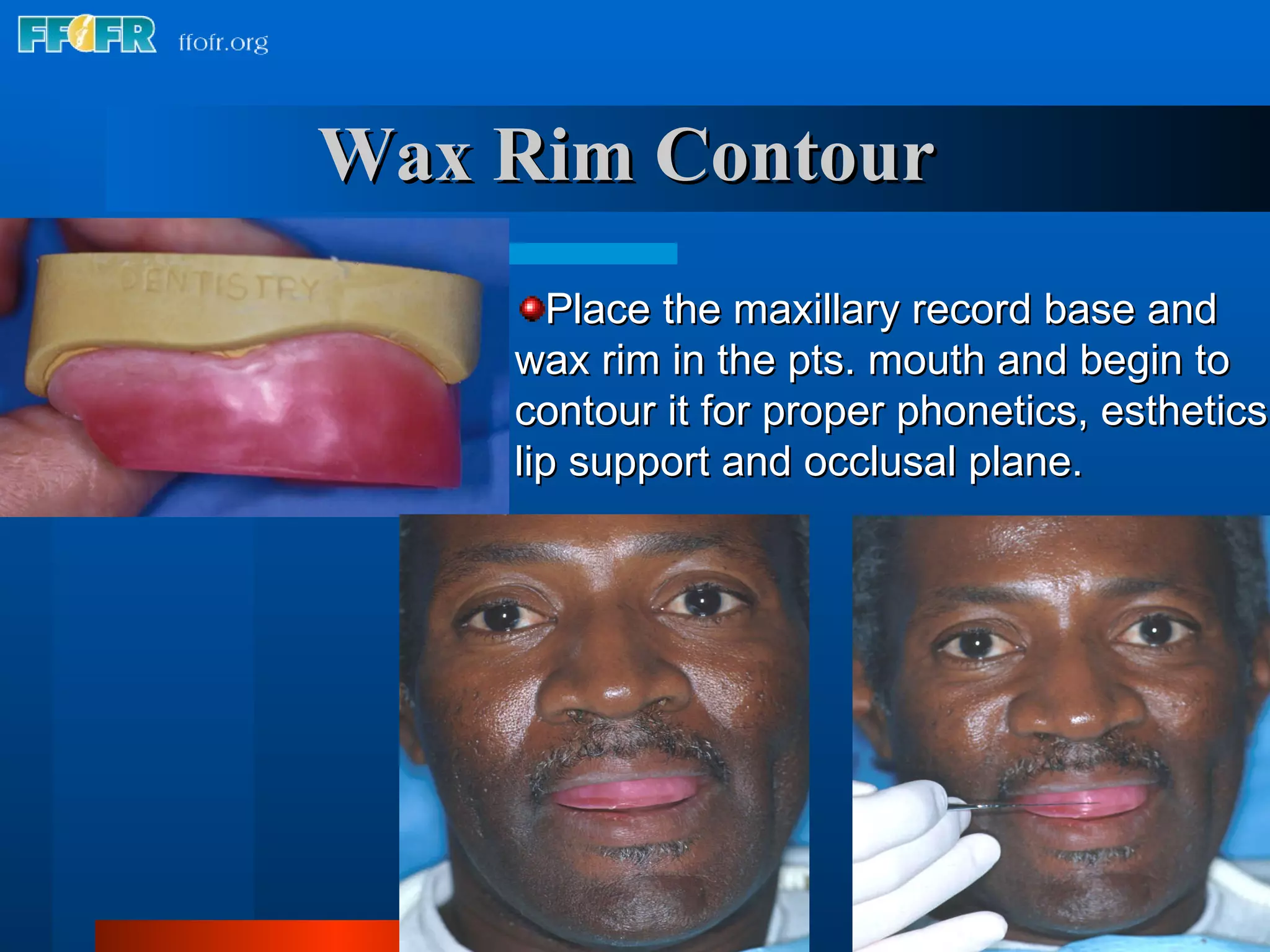
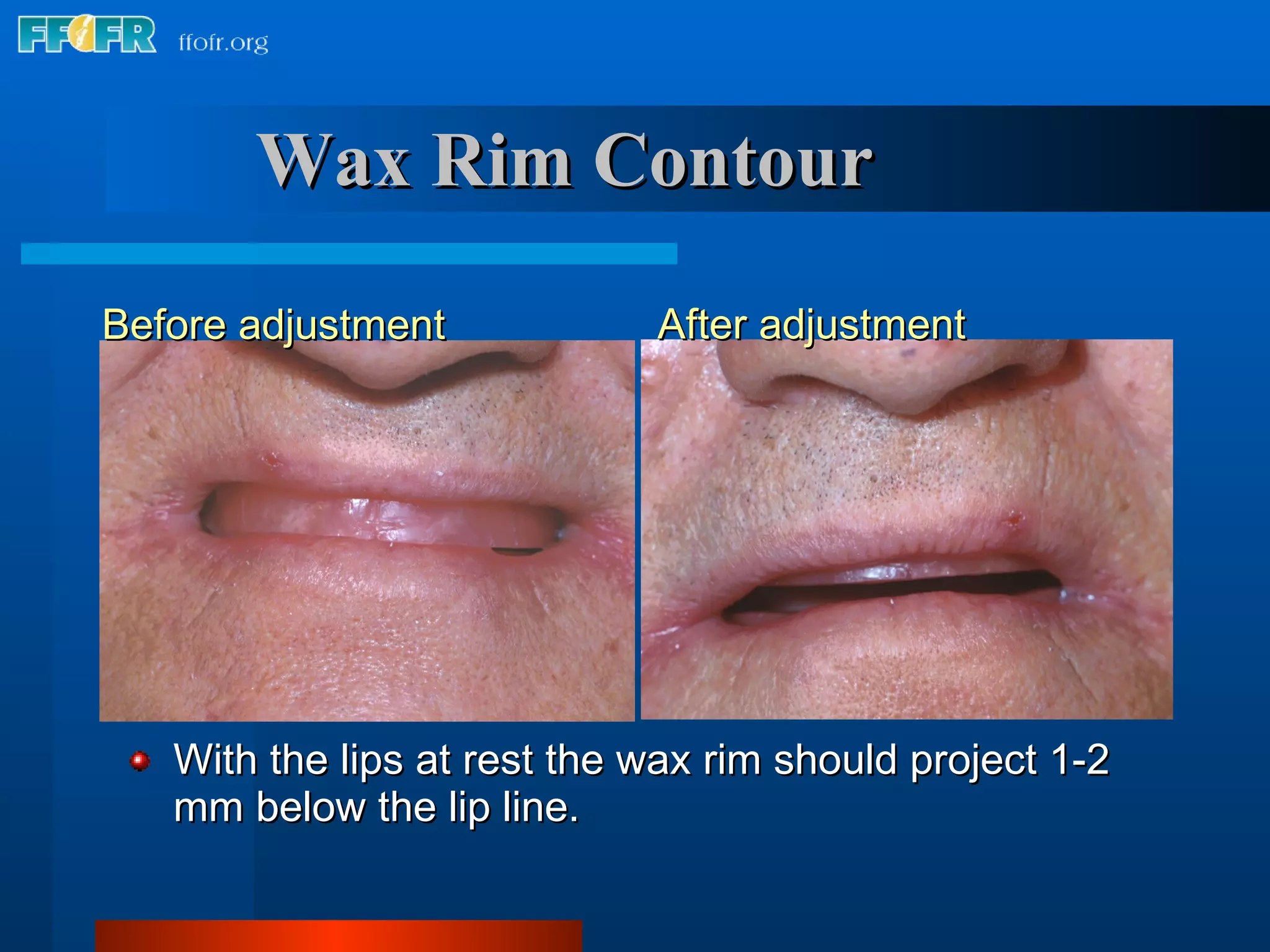

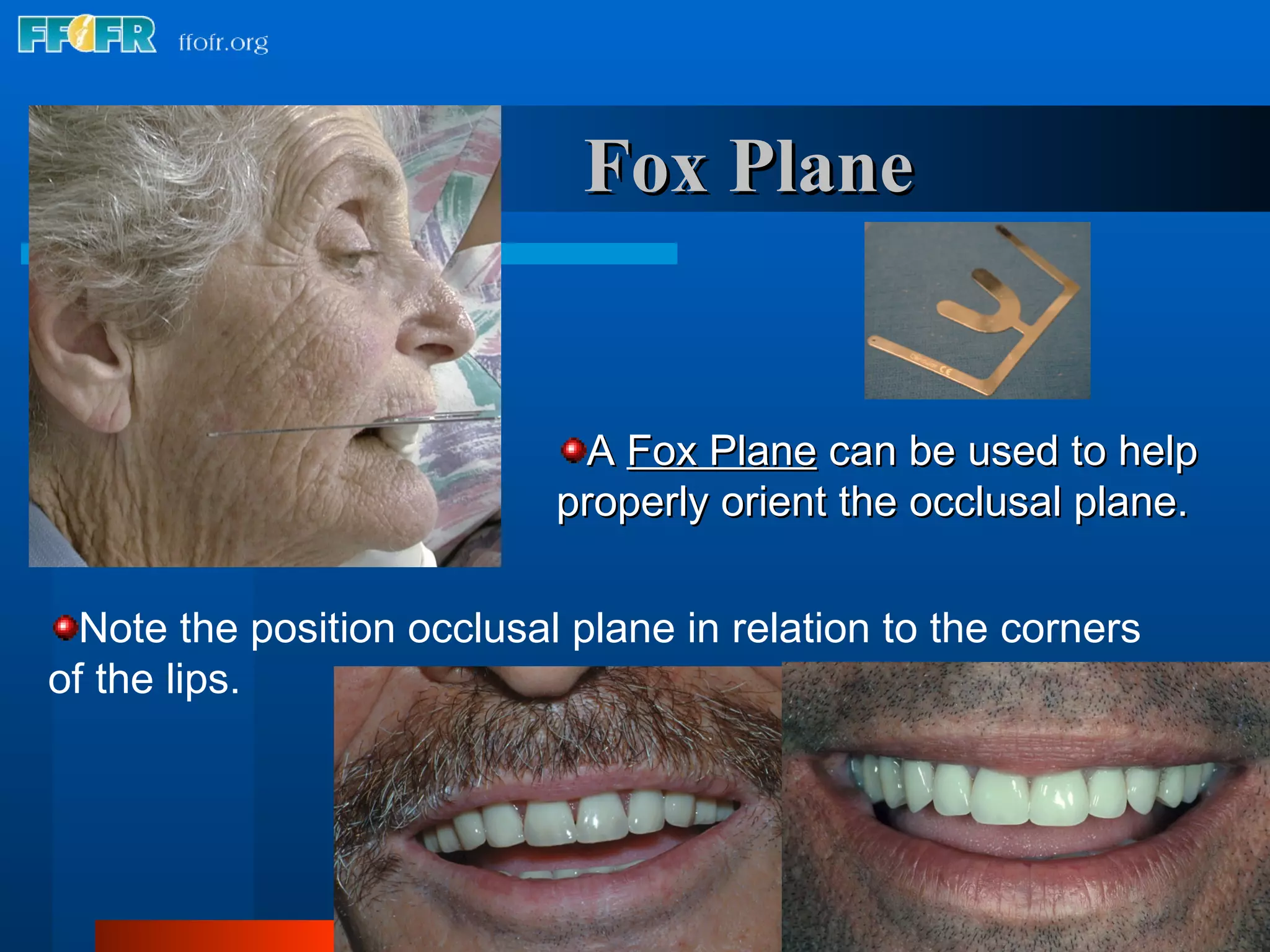

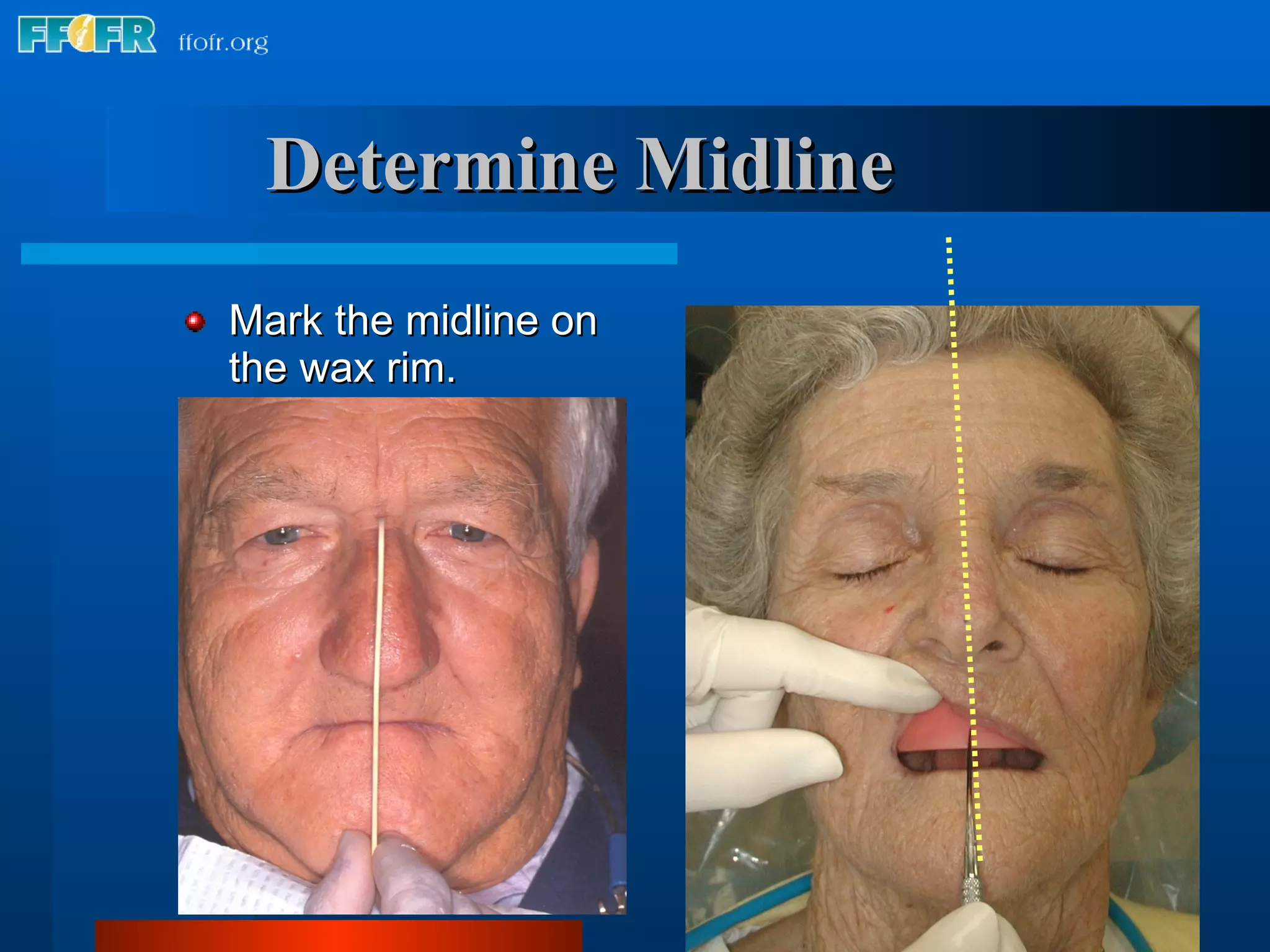



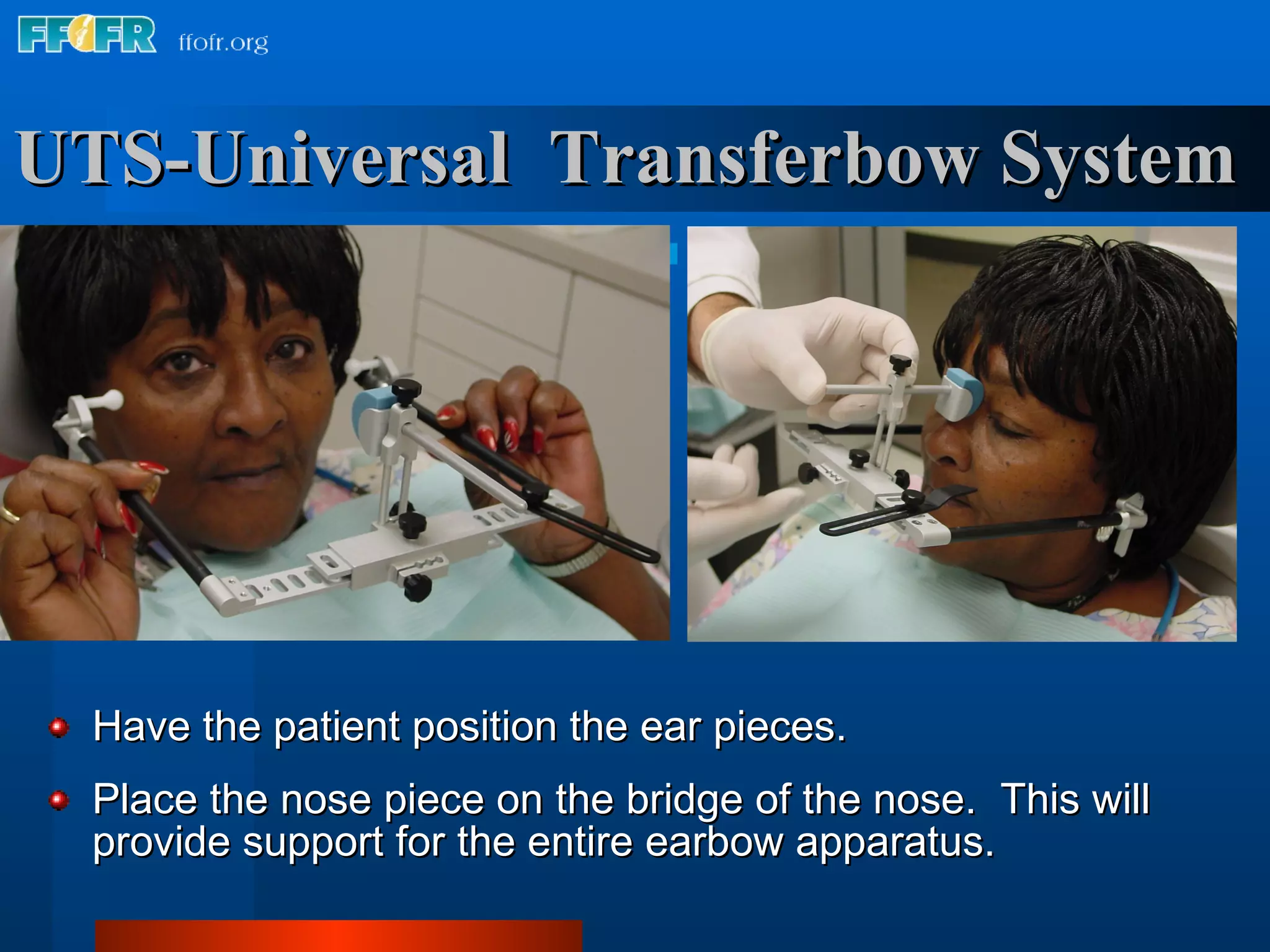






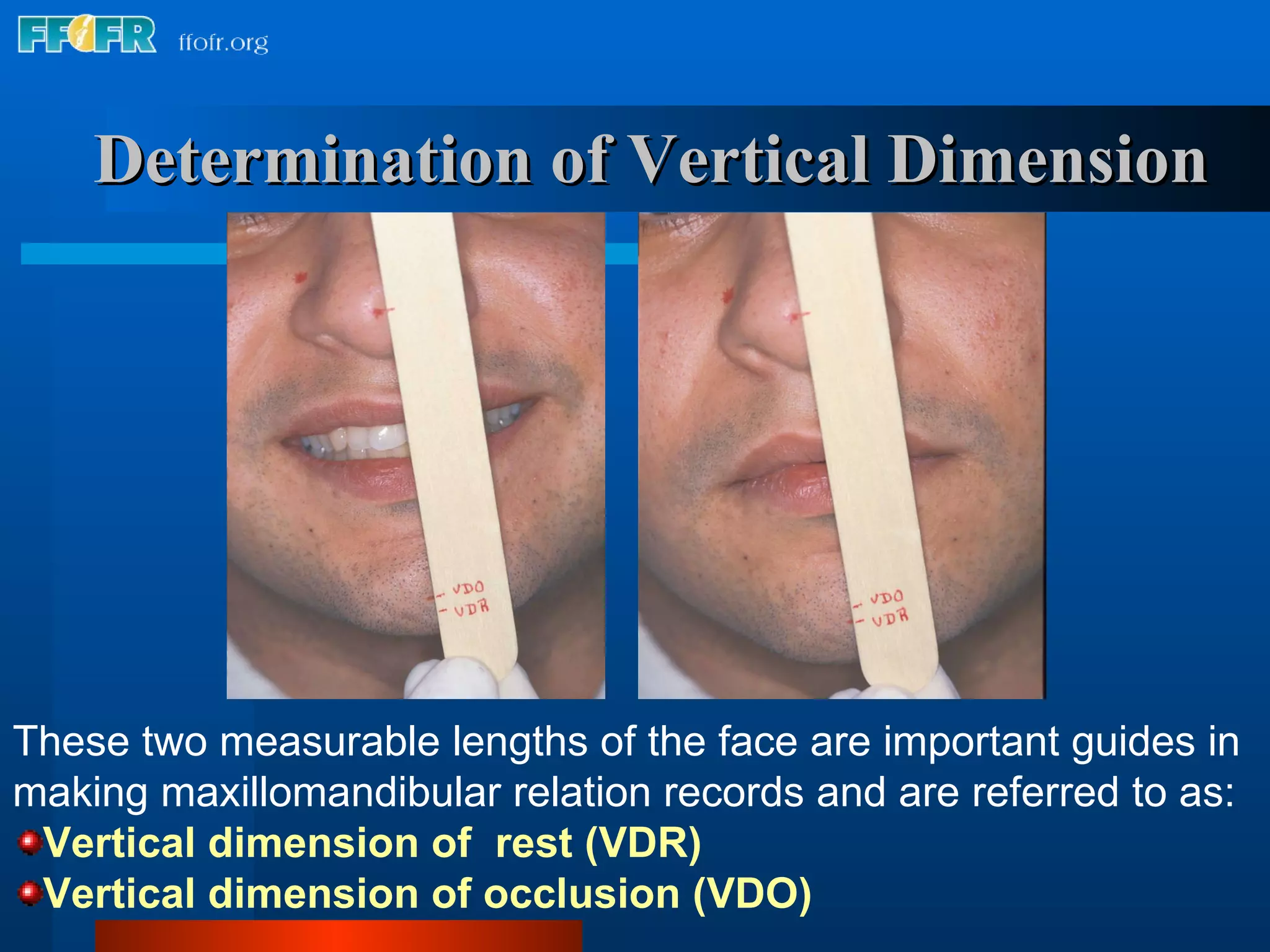


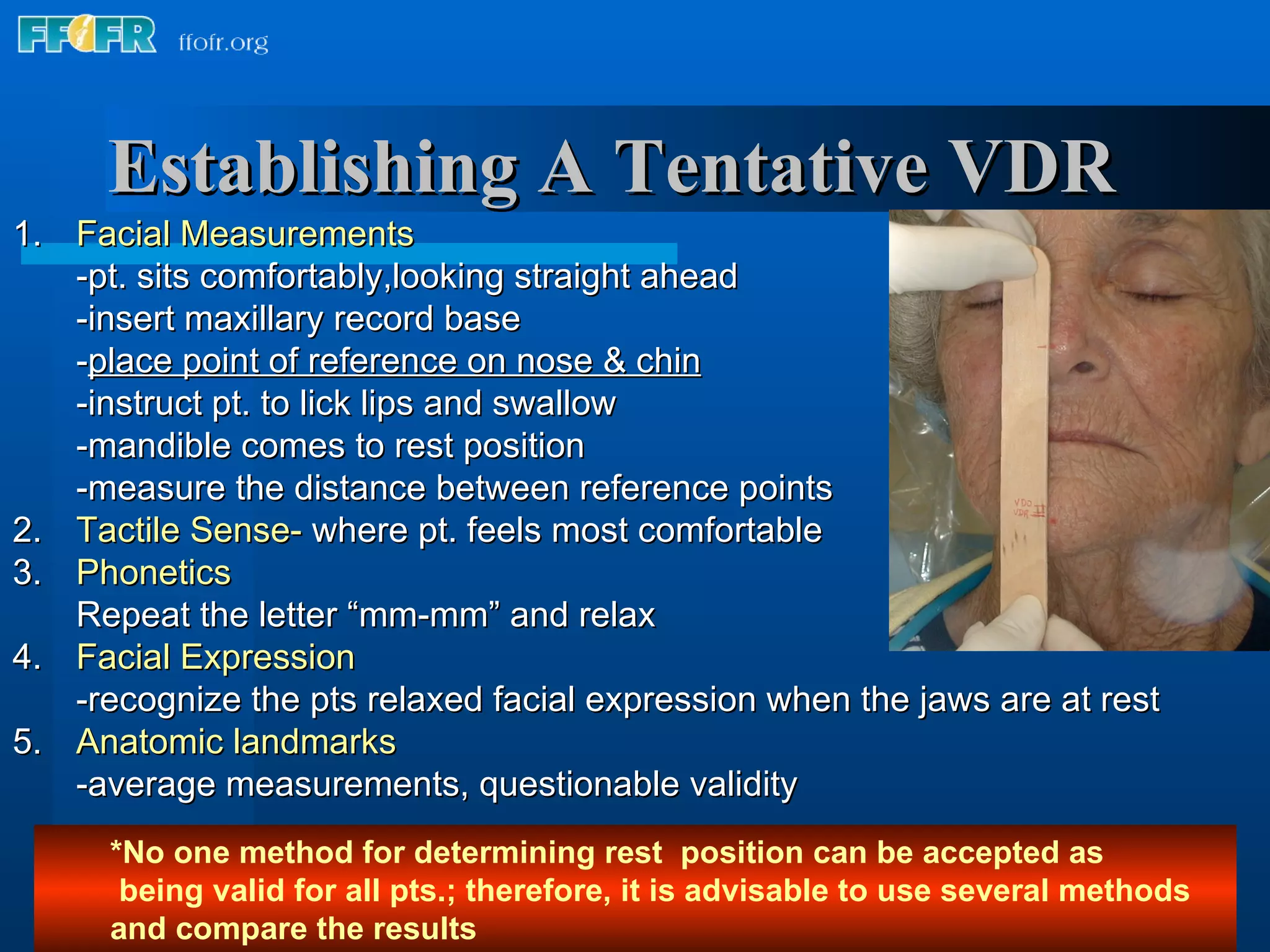
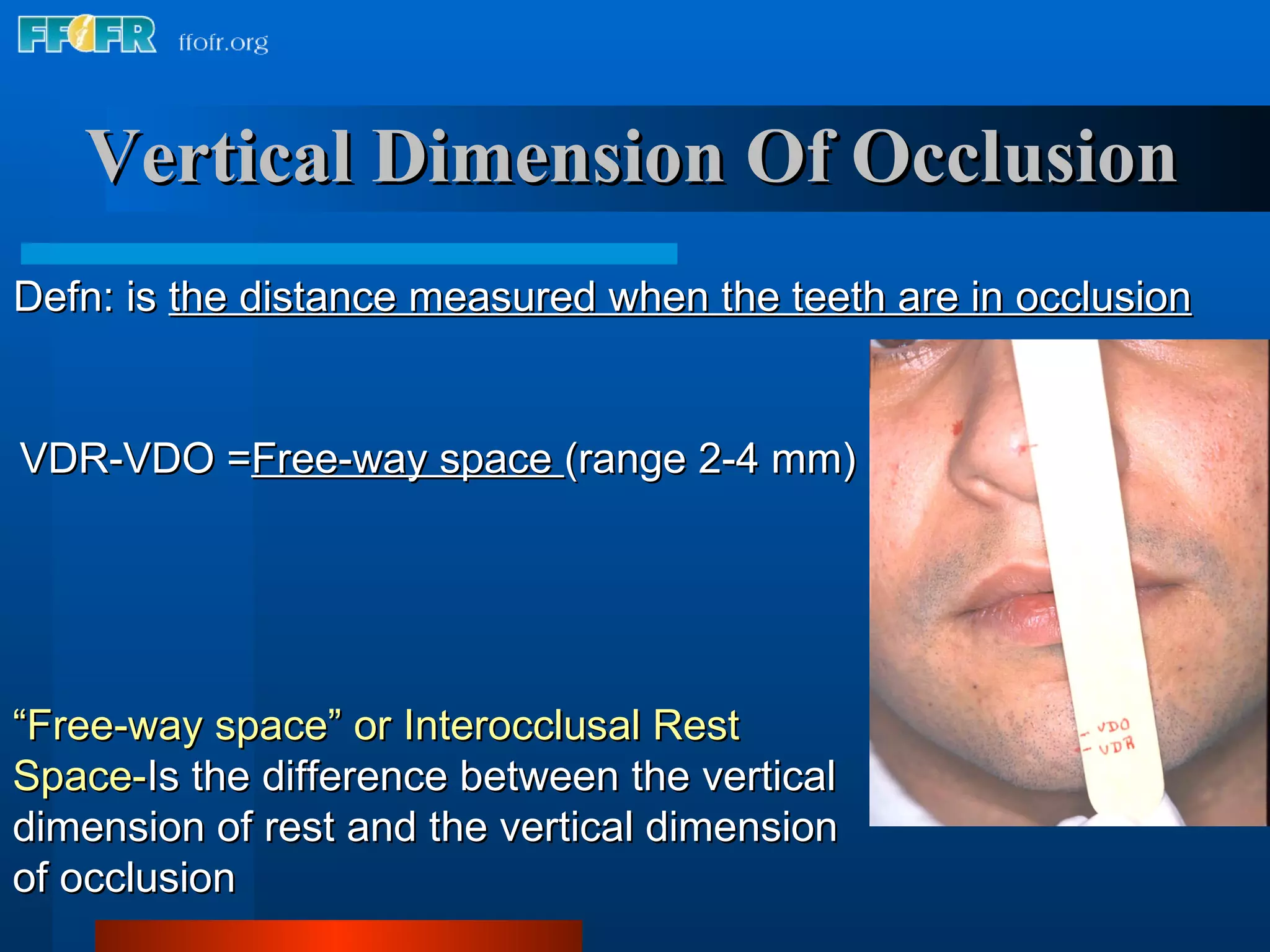


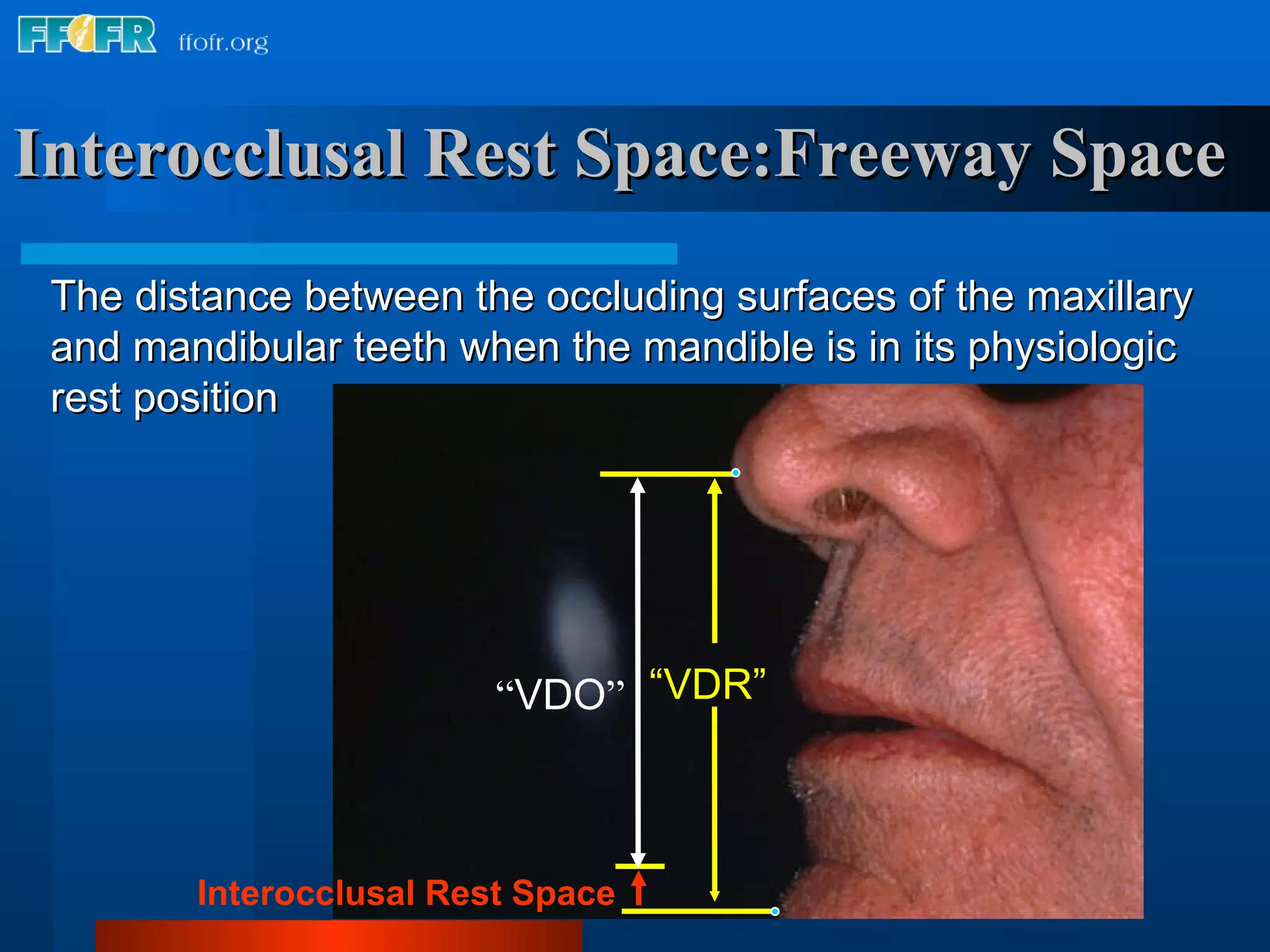



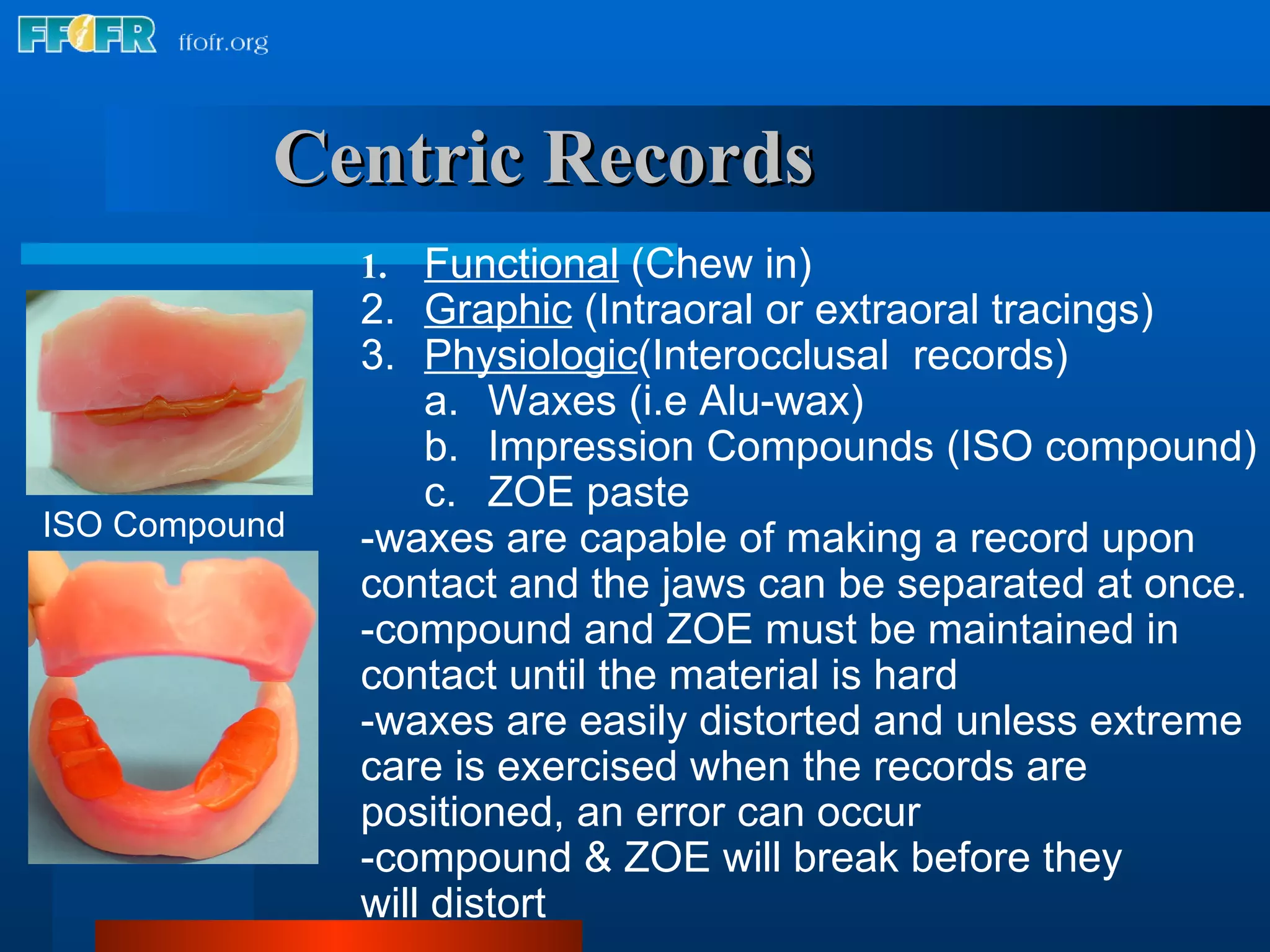


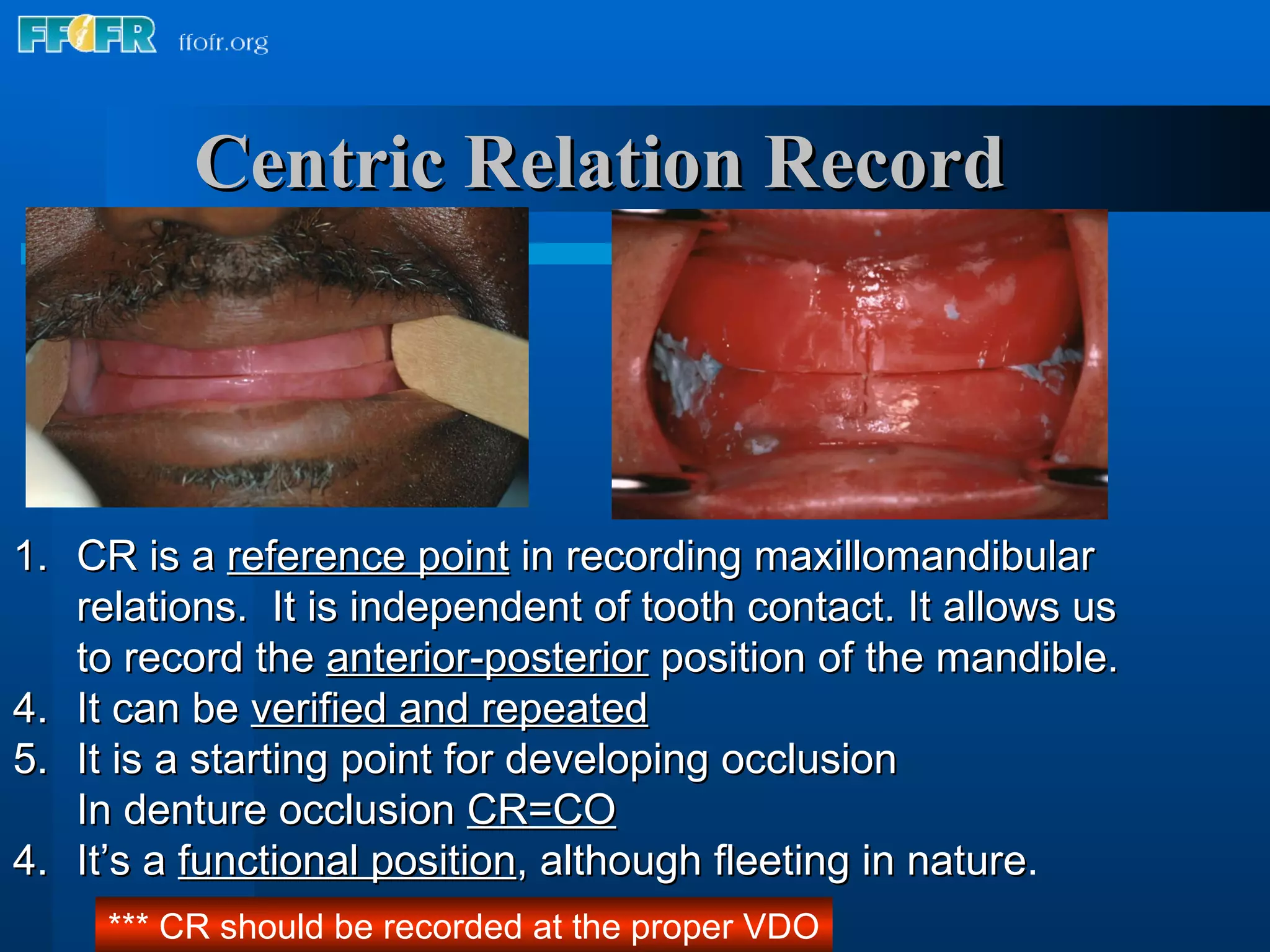
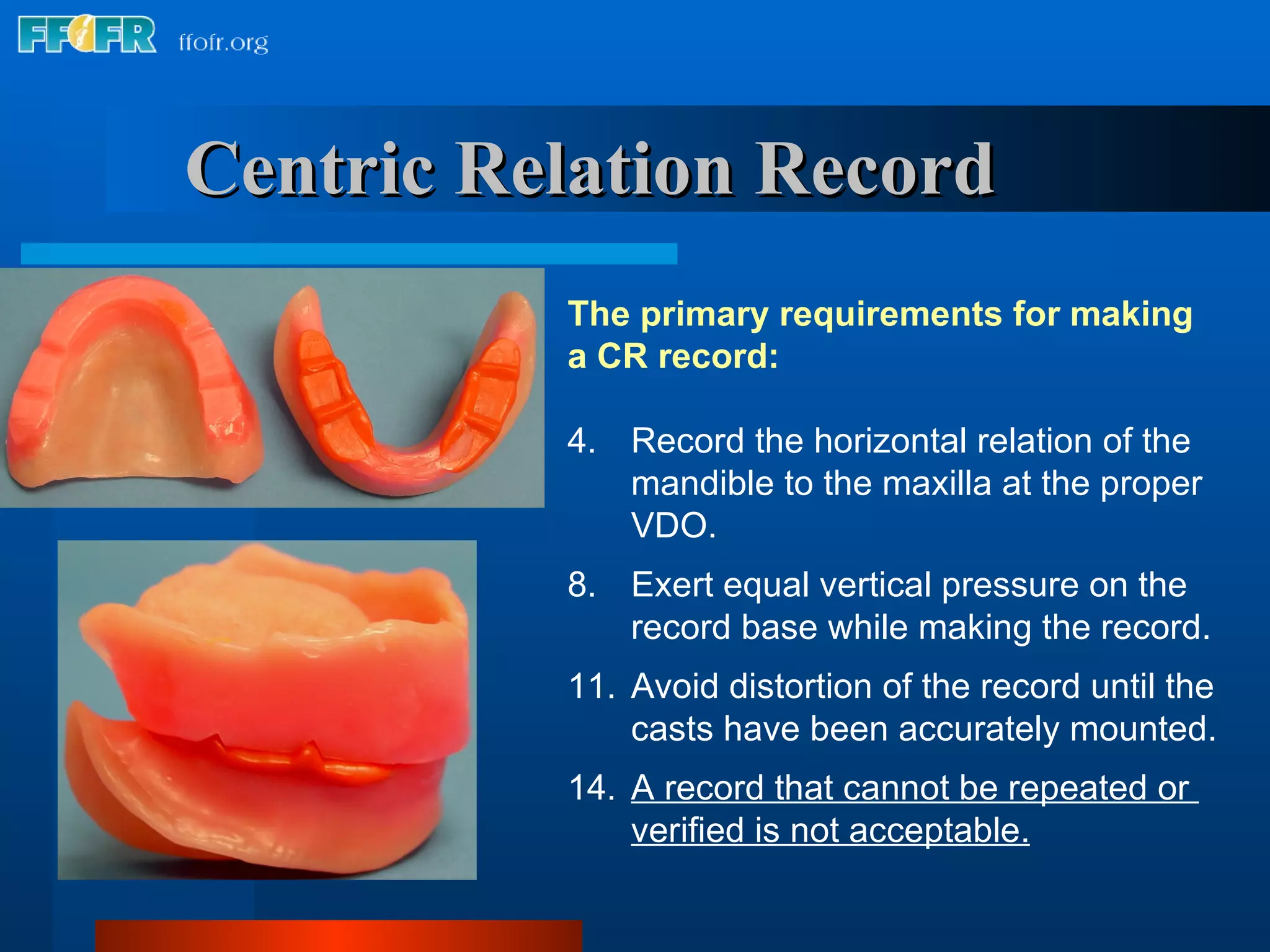


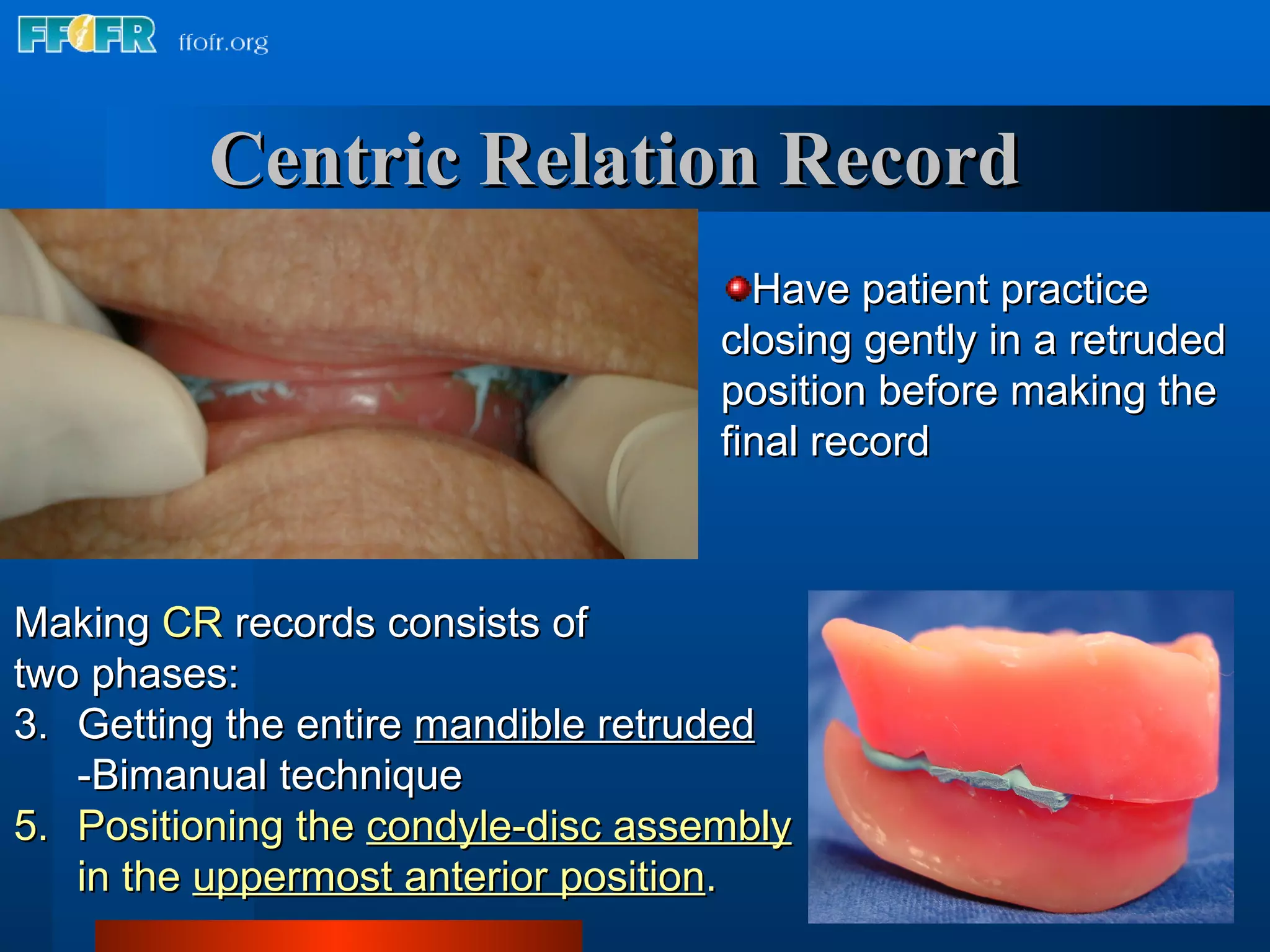












The document discusses various methods and considerations for making maxillo-mandibular relation records to transfer a patient's jaw relationship to an articulator. It covers determining and recording the vertical dimension of rest and occlusion, using a facebow to transfer maxillary orientation, and different materials that can be used to make centric relation records like waxes, impression compounds, and ZOE paste. The goal is to establish a balanced occlusion on the articulator that limits trauma to supporting structures and restores function.




















































![vertical jaw relation [Autosaved].pptx .](https://cdn.slidesharecdn.com/ss_thumbnails/verticaljawrelationautosaved-250920192706-cb5ca831-thumbnail.jpg?width=640&height=640&fit=bounds)











































