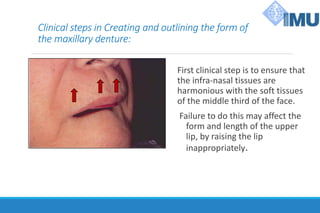
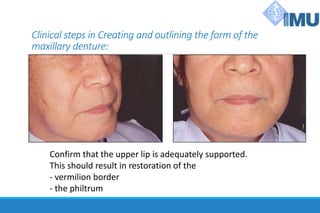
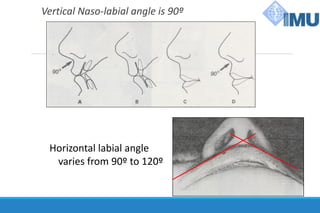
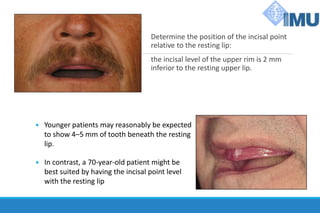
1. Maxillo-Mandibular Relation (MMR) involves creating and outlining denture forms, recording intermaxillary relations in centric relation, and selecting teeth.
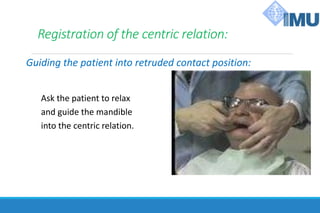
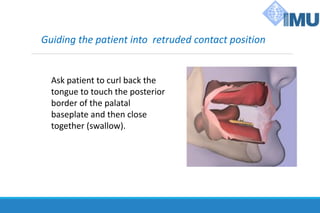
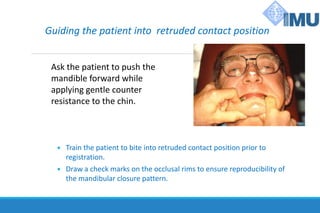
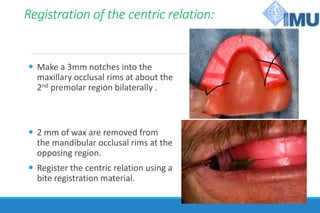
2. Recording intermaxillary relations in centric relation involves guiding the patient to retruded contact position and making impressions to capture the mandibular arc of closure.
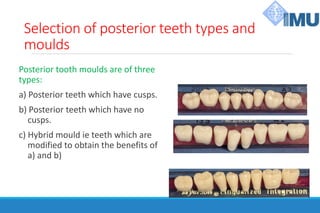
3. Selection of teeth involves choosing anterior teeth to restore lip contours and smile lines and posterior teeth types and shades based on facial features and patient preferences.