WHY IS RECORDINGOF JAW RELATIONS
IMPORTANT ???
To design the dentures in such a way
that they function in harmony with
the 2 jaw bones and the joint in
between them i.e., the
Temporomandibular joint
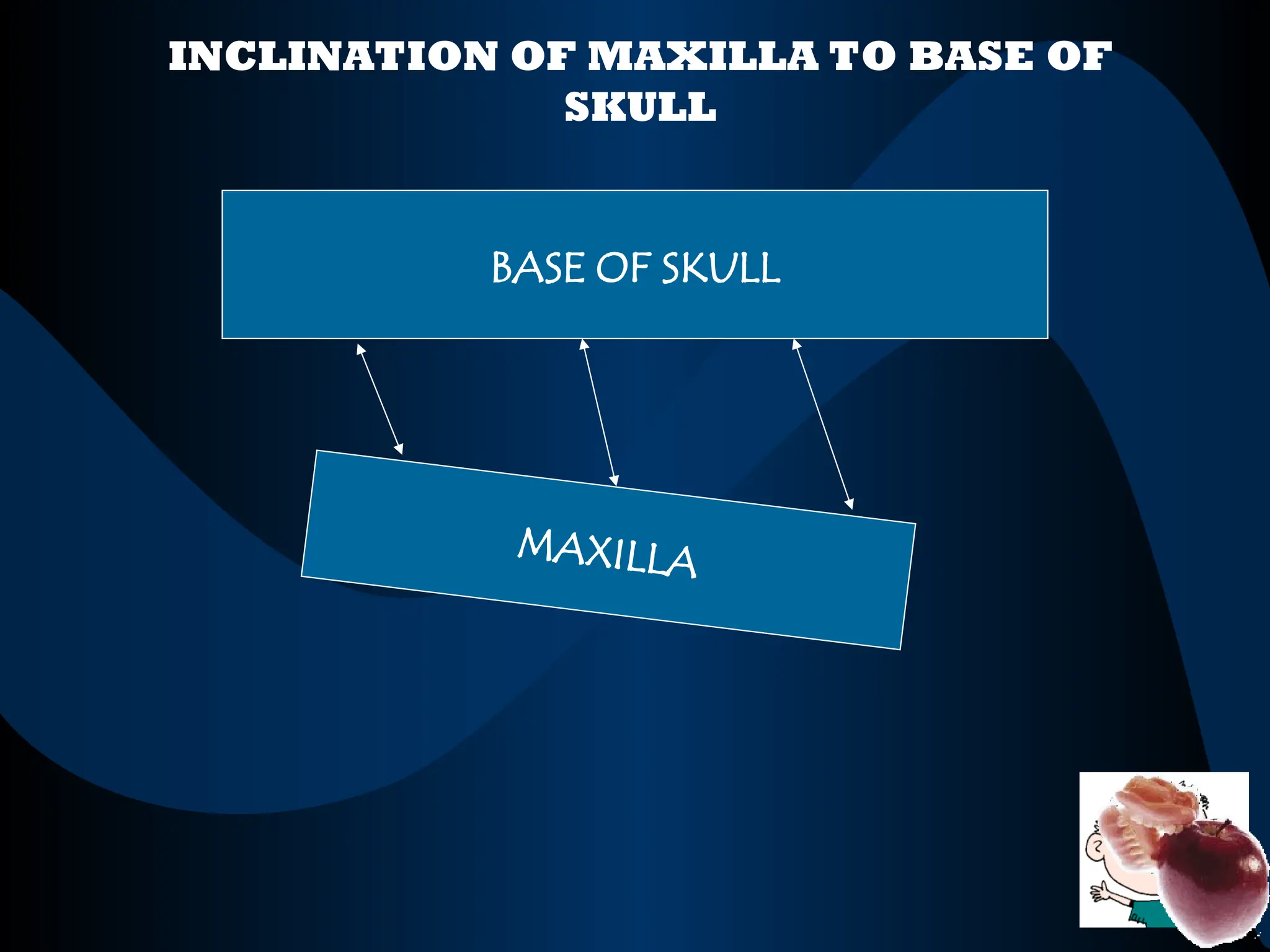
“The orientation ofthe maxilla to the
base of cranium and to the imaginary
transverse axis passing through the
center of the condyles around which
the mandible may rotate within the
sagittal plane ”
ORIENTATION JAW RELATION
9.
VERTICAL JAW RELATION
Itinvolves the establishment of vertical
dimension of the dentures in harmony
with the appearance of the face , for
maximum functional efficiency and
patient comfort
10.
HORIZONTAL JAW RELATION
Itinvolves the relationship of mandible
to the maxillae in the horizontal plane
at centric and eccentric positions
Can be recordedwith the help of a
FACE-BOW device
“Face-bow is a caliper like device used
to record the spatial relationship of the
maxilla to the opening axis of TMJ and
the base of skull and then transfer the
maxillary cast in the same relationship
to the opening axis of articulator”
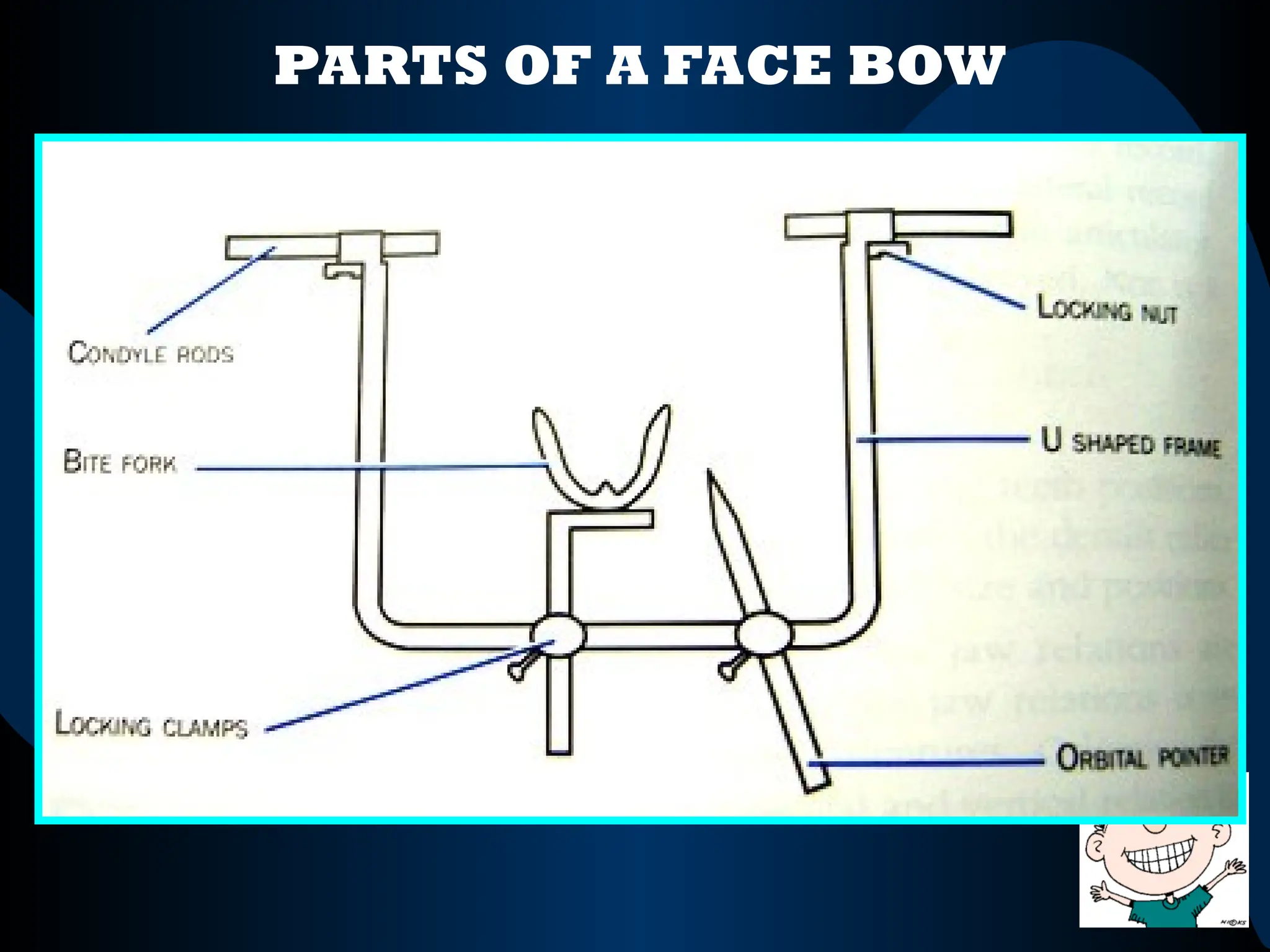
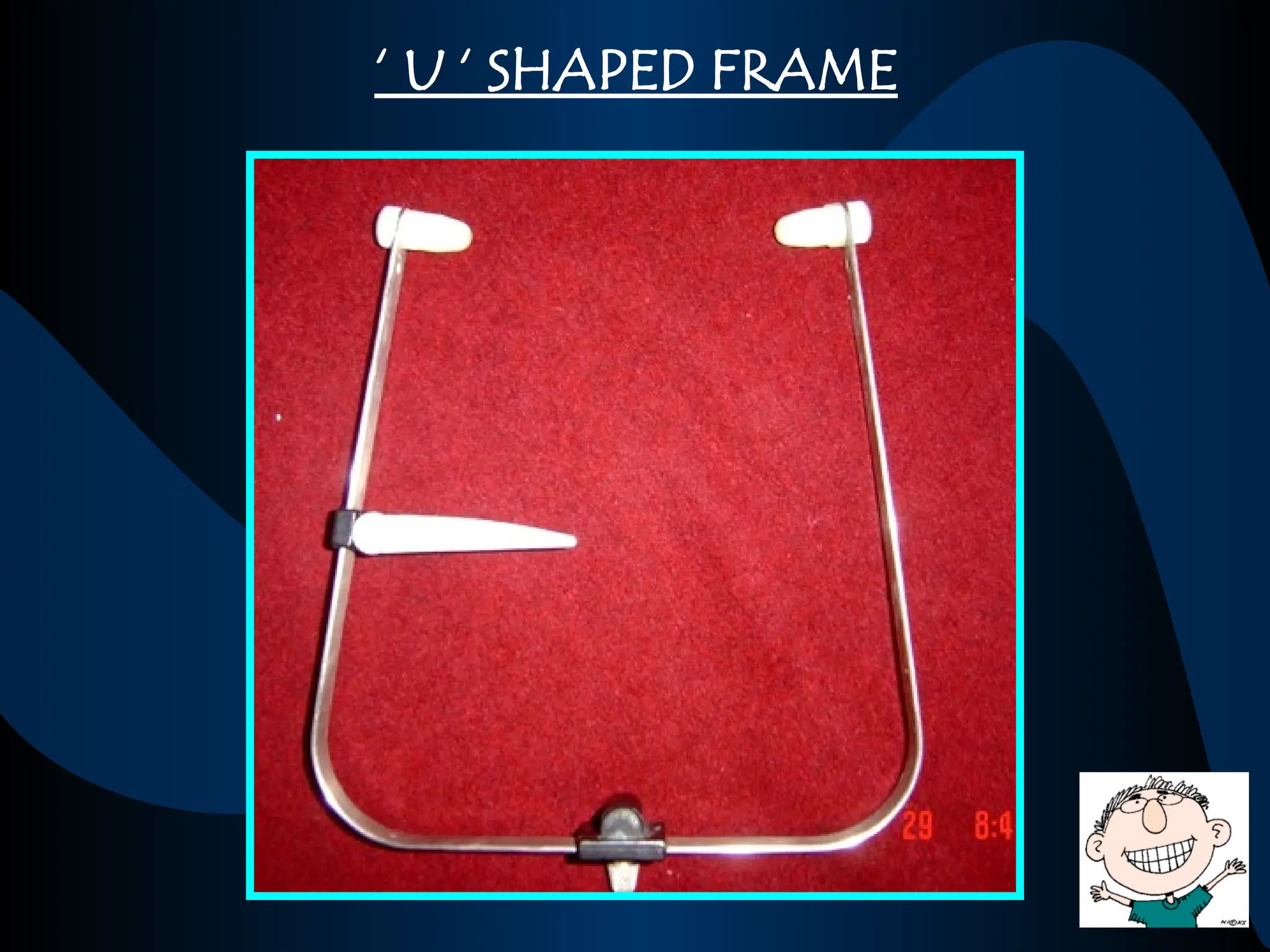
Forms the mainframe of the face bow
Records the plane of the cranium
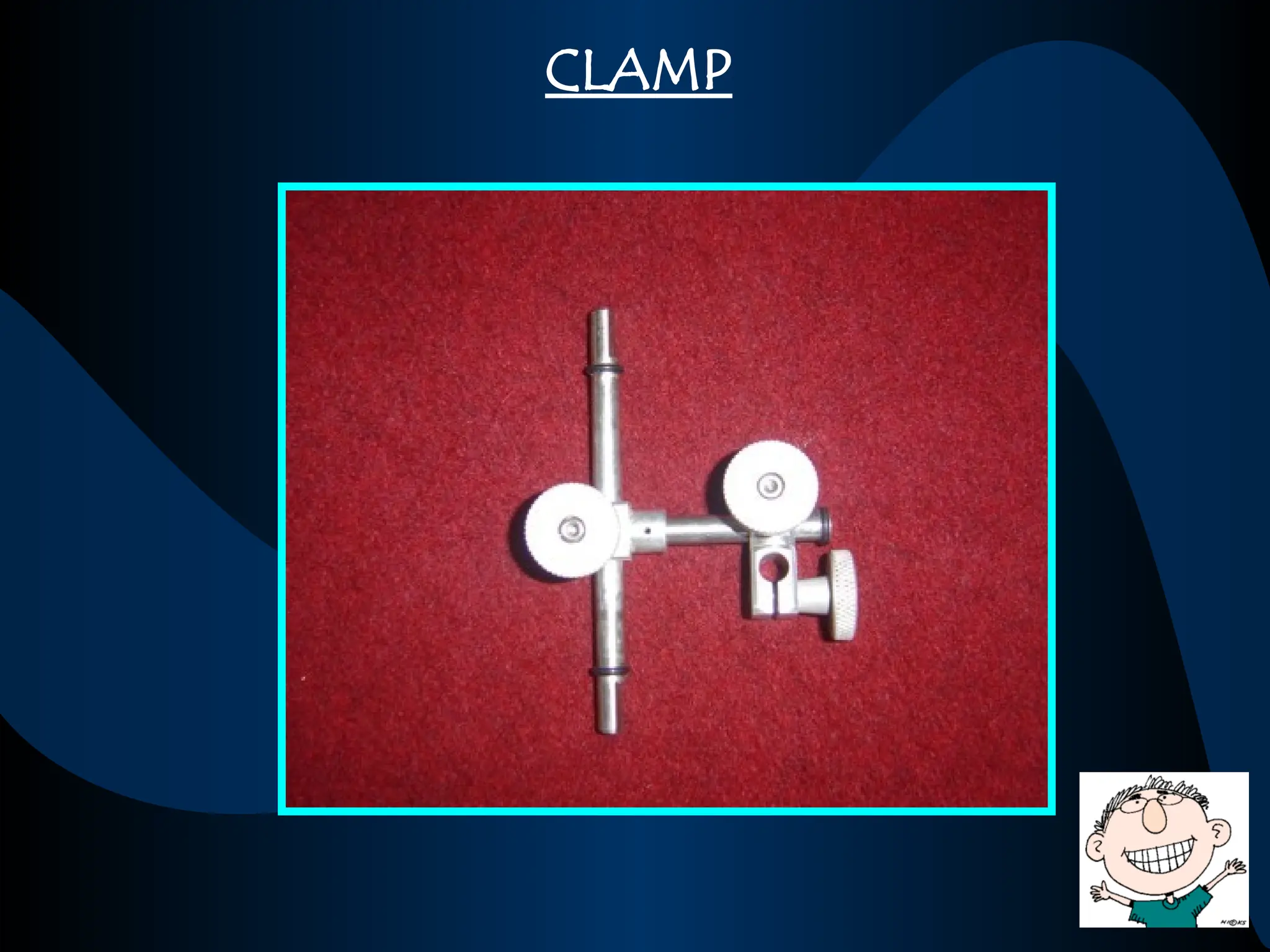
All other components are attached to
this frame with the help of clamps
19.
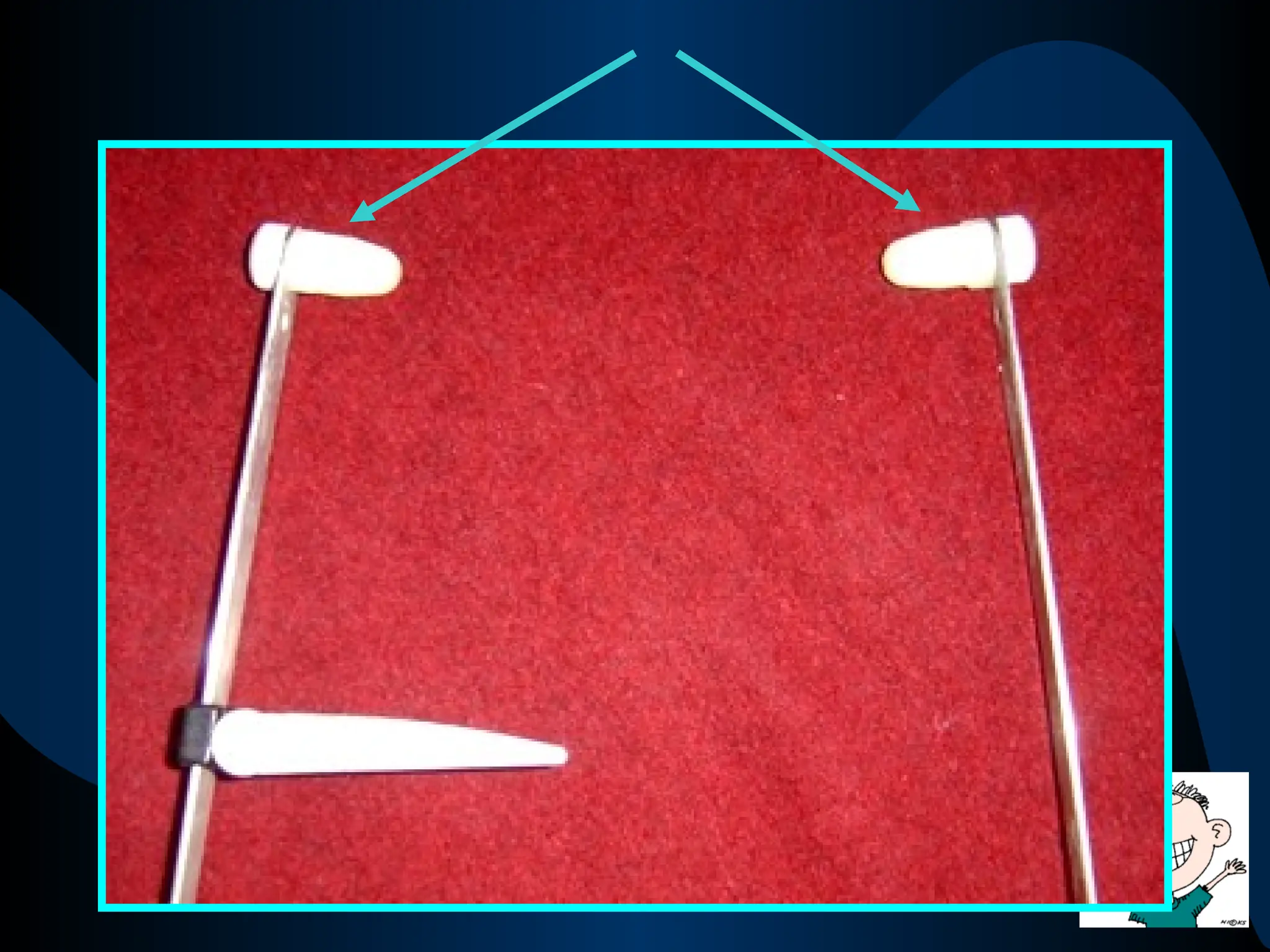
EAR PIECES /PLUGS
2 small plastic plugs that fit the external
auditory meatus
Help to locate the opening axis of the
Temporomandibular joint / Hinge Axis
TYPES OF FACEBOW
Arbitrary Face bow
Fascia type
Ear piece type
Self centering Manual centering
Kinematic Face bow
Hanau spring bow
33.
Once the maxillais oriented to the
opening axis on the face , the entire
assembly is attached to the articulator
to transfer the maxillary cast on the
articulator in the same relationship to
the opening axis of the articulator
Vertical Jaw Relations/Dimensionsare
expressed in terms of amount of
separation of maxillae and mandible
under specified conditions ,as viewed in
the frontal plane
37.
Vertical Jaw Relations/Dimensionscan
be classified into 2 types
Vertical
Dimension of
Rest
Vertical
Dimension of
Occlusion
Occlusion
38.
Vertical Dimension ofOcclusion (VDO)
When the natural teeth are present and in
occlusion ,the VDO is maintained or
established by them
When the natural teeth are lost & the patient
wears dentures, the VDO is established by
the two dentures when the teeth are in
contact
“The amount of separation of the jaws
when the teeth are in occlusion”
39.
Therefore , theVDO must be
established for edentulous patients, such
that their denture teeth will come into
contact at the appropriate height
40.
Vertical Dimension ofRest (VDR)
“The amount of separation of the jaws
when the mandible is in a
Physiologic Rest Position”
It is the position where the muscles that close
the jaws and those that open the jaws are in a
state of minimal contraction [function], just
enough to maintain the posture of mandible
41.
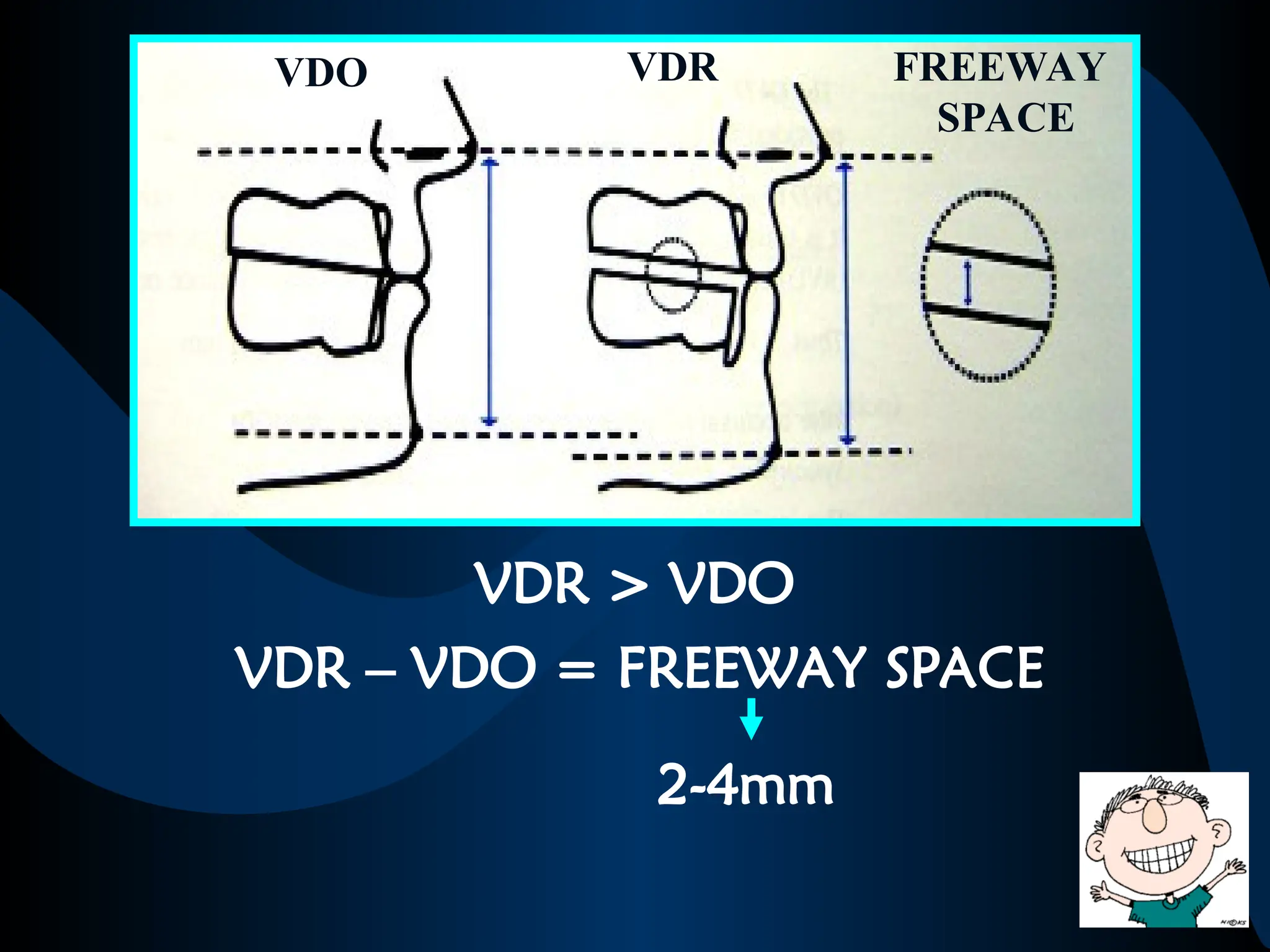
VDR > VDO
VDR– VDO = FREEWAY SPACE
VDO VDR FREEWAY
SPACE
2-4mm
42.
IMPORTANCE OF FREEWAYSPACE
•Assessing the vertical dimension of
occlusion of dentures
If the freeway space is < 2mm , it indicates
that the VDO is increased
If the freeway space is > 4mm , it indicates
that the VDO is decreased
43.
•Relaxation of masticatoryapparatus
and denture bearing areas
At rest position , when the teeth are not in
contact & freeway space is adequate, there is
no strain on the TMJ and minimal activity of
elevator and depressor muscles of the mandible
Allows for relaxation of the muscles and TMJs
and avoids fatigue
44.
At the sametime , if the dentures have no /
inadequate freeway space , the denture bearing tissues
are continuously and excessively loaded
Resorption of bone is aggravated
45.
Methods for DeterminingVertical
Dimension
Mechanical methods
Preextraction records
Ridge relations
Measurement of former
dentures
Physiologic methods
Physiologic rest position
Phonetics
Swallowing methods
Tactile sense & patient comfort
PRE-EXTRACTION METHODS
Profile radiographs
Canbe used to assess the vertical dimension of
occlusion before extraction
The vertical dimension existing before the
removal of teeth can be used as a guide
establishing vertical dimension of the dentures
48.
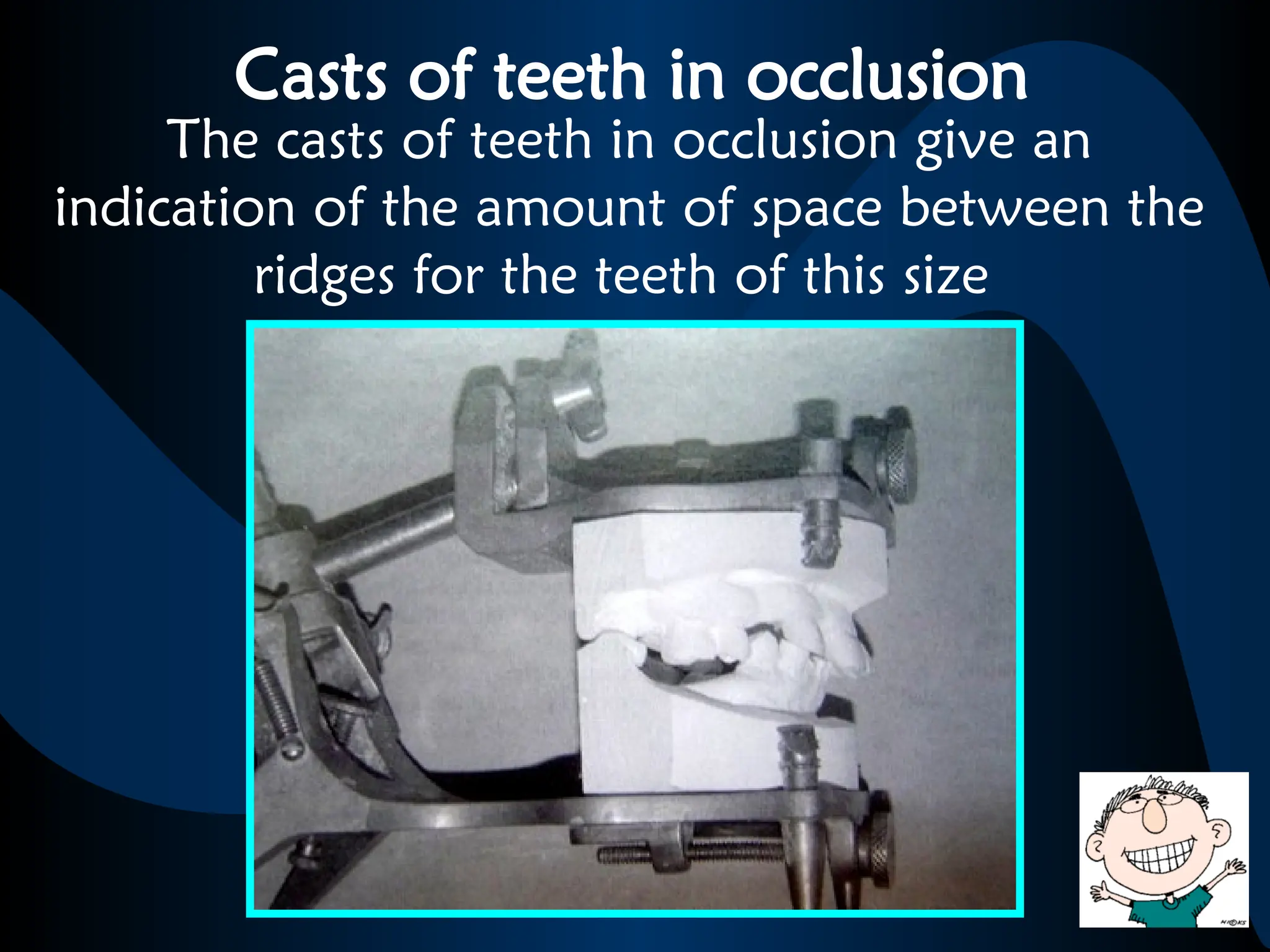
Casts of teethin occlusion
The casts of teeth in occlusion give an
indication of the amount of space between the
ridges for the teeth of this size
49.
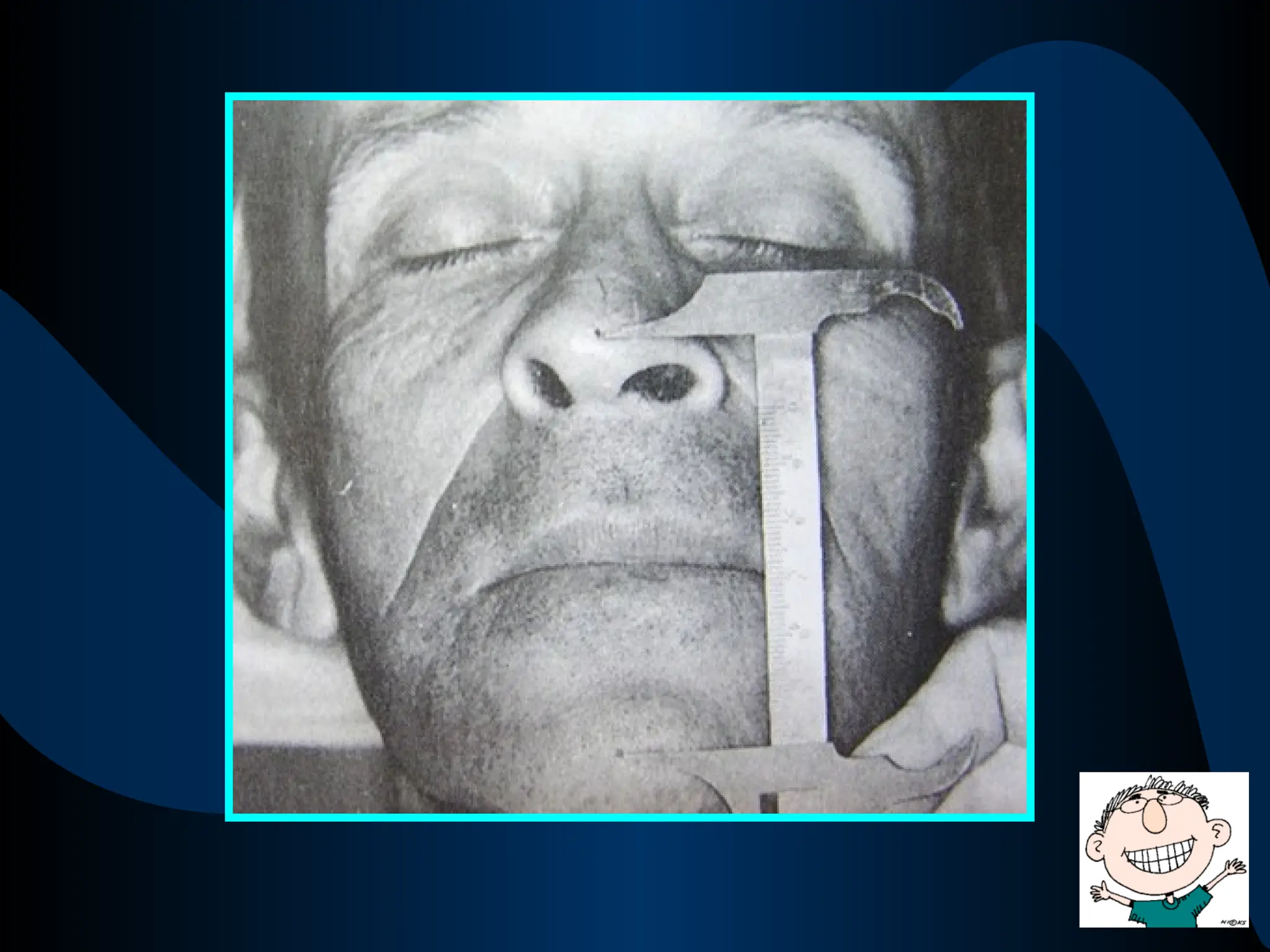
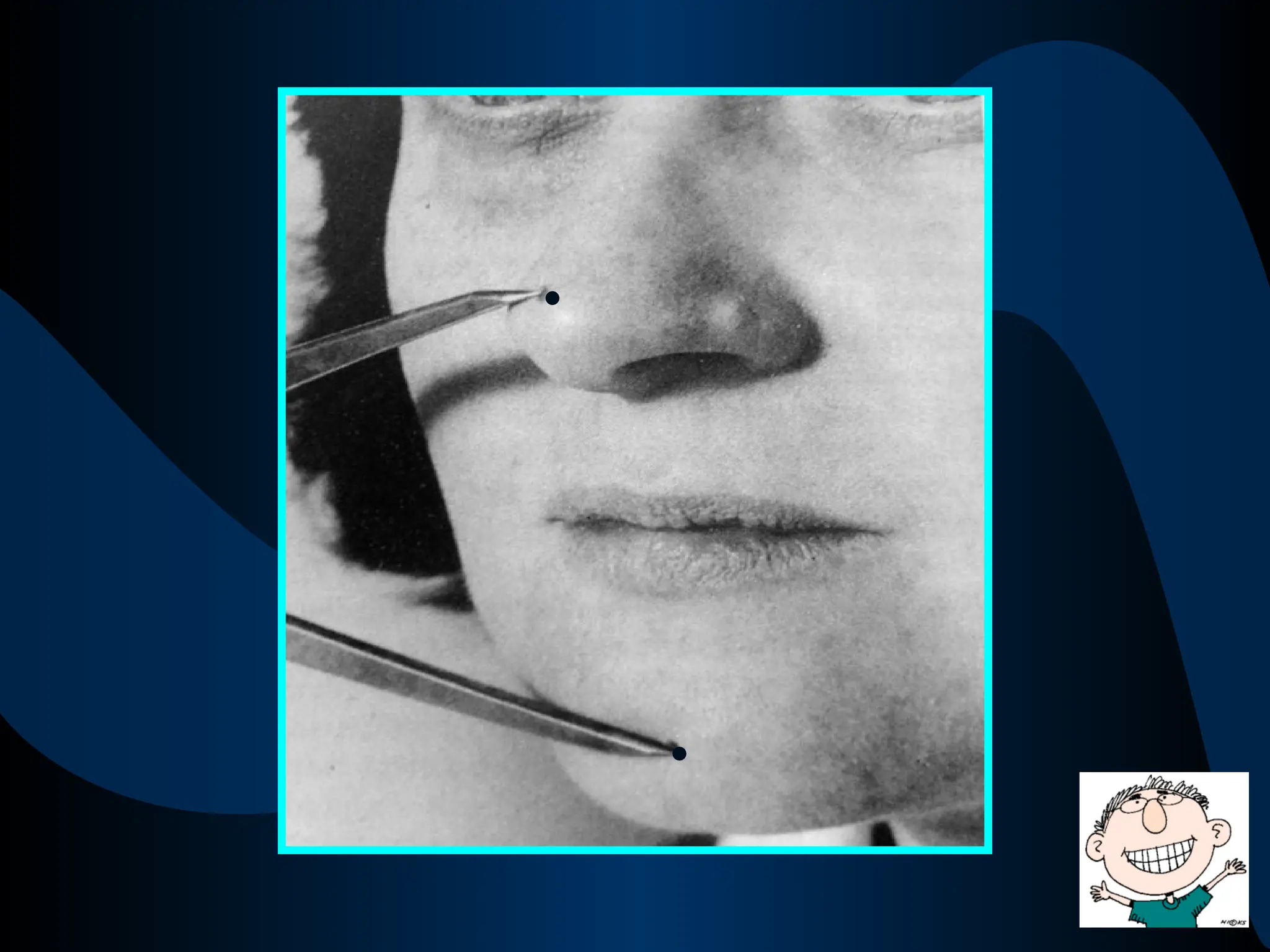
Facial measurements
Devices likecalipers or pair of dividers can be
used to make measurements in the middle &
lower 3rd
of the face e.g., from the base of the
nose to the base of the chin , before the
extraction of the teeth
These measurements can be used to establish
the same dimensions during denture fabrication
52.
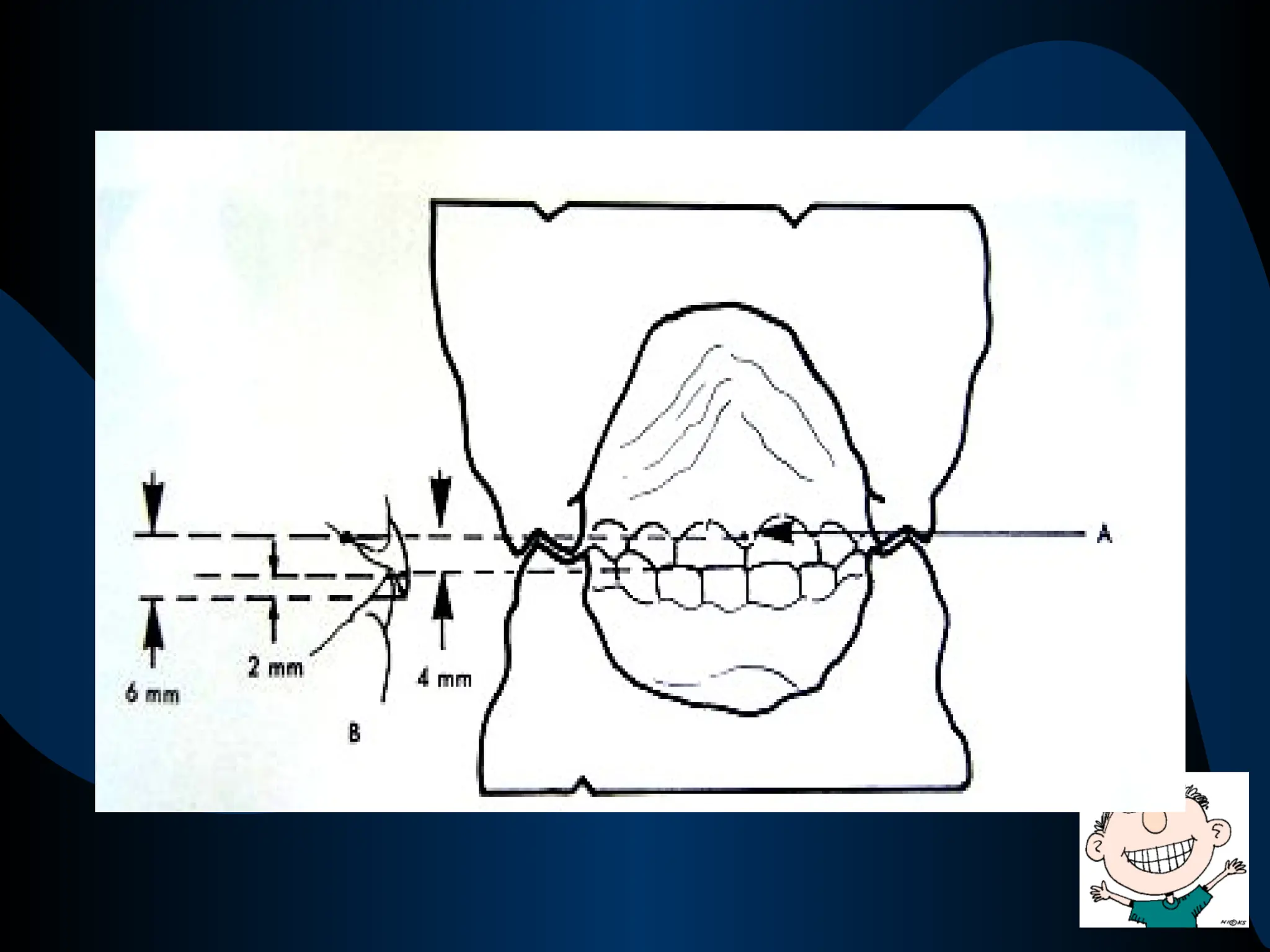
RIDGE RELATIONS
Incisive papillato mandibular incisors
The distance of papilla from the incisal
edges of the mandibular incisors averages
approximately 4mm in natural dentition
The distance of papilla from the incisal
edges of the maxillary incisors averages
approximately 6mm in natural dentition
54.
Therefore the meanvertical overlap of
the opposing incisors is about 2mm
Parallelism of themaxillary & mandibular
ridges , plus a 5-degree opening in the
posterior region, often gives a clue as to
the appropriate amount of jaw separation
57.
Parallelism of themaxillary & mandibular
ridges is natural
Parallelism of the maxillary & mandibular
ridges is favorable from a mechanical
point of view to prevent any
anteroposterior sliding of dentures during
function
58.
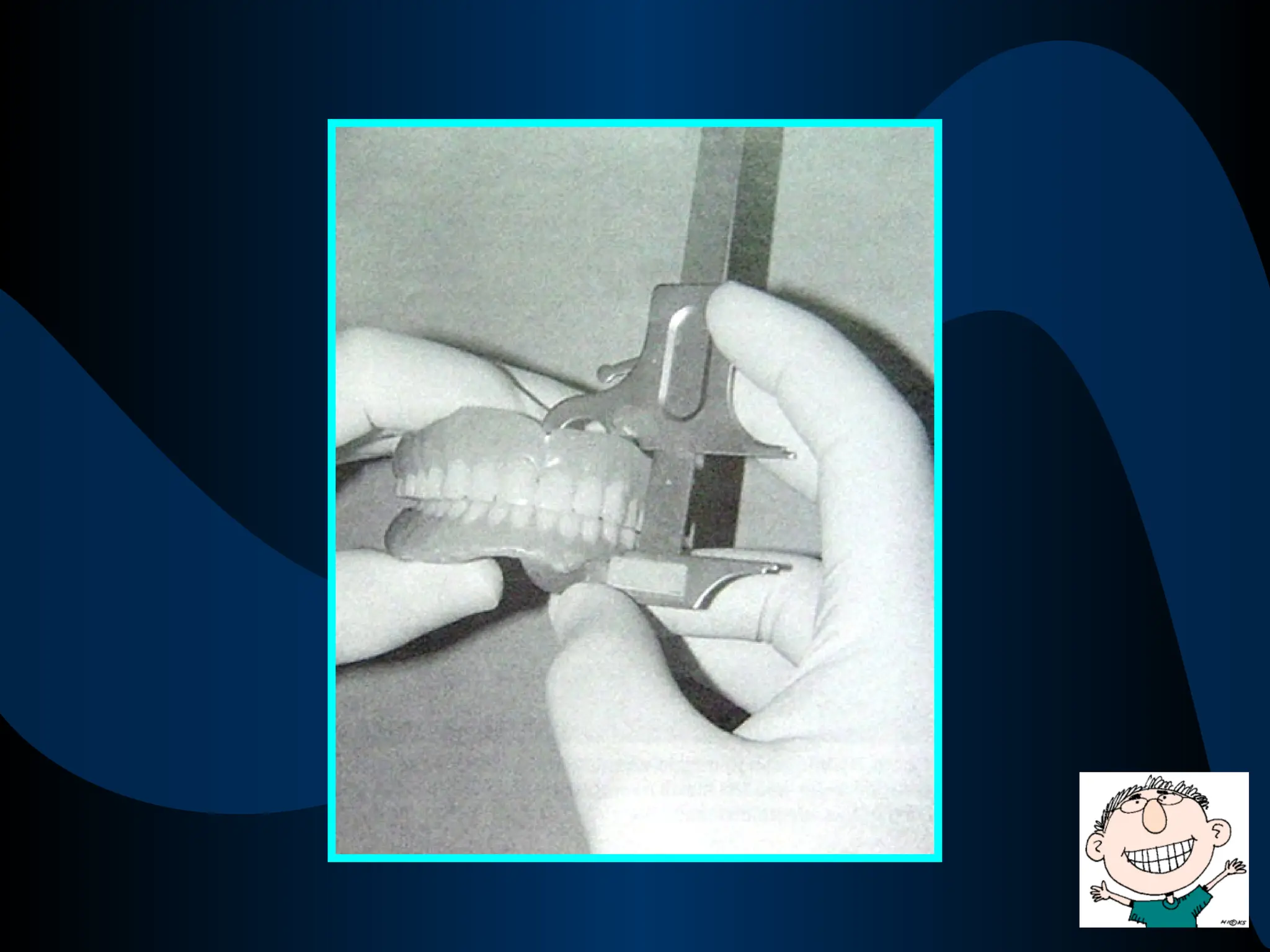
Measurement of formerdentures
Measurements can be made between the ridge
crests of the maxillary and mandibular dentures
with a Boley gauge
If the observations on the patients face indicate
that this distance is too short or too long , a
corresponding change can be made in the new
dentures
PHYSIOLOGIC REST POSITION
Registrationof the jaw in physiological
rest position gives an indication of the
vertical dimension of occlusion
At the physiological rest position , there
should be a freeway space of 2-4mm
between the occlusal rims
62.
This may notbe an exact guide ;
therefore has to used in concordance with
other methods
63.
PHONETICS
Phonetic tests includelistening to speech
sound production & observing the
relationships of teeth during speech
The production of ch, s, & j sounds brings
the anterior teeth close together and
almost touch each other but do not touch
64.
If the distancebetween the upper & lower
incisors is too large , it indicates that the
VDO is too small
If the anterior teeth touch when these
sounds are made / click together during
speech , it indicates that the VDO is too
large
65.
SILVERMAN’S CLOSEST SPEAKINGSPACE
Similar to the technique of phonetics
where ‘S’ sounds are used to assess the
vertical dimension
Range of 2-11 mm depending on the
functional range of the patient
66.
The Freeway Space& Closest Speaking
Space are not the same
The freeway space is an assessment of VD
at rest ; while the speaking space is an
assessment of VD during function
67.
ESTHETICS
The vertical relationof the mandible to
the maxillae also affects esthetics.
Normally the tone of the facial skin
should be the same throughout and for
this an appropriate vertical dimension is
necessary
68.
If the verticaldimensions of the dentures
is excessive , it will lead to stretched
appearance of the facial skin
If the vertical dimensions of the dentures
is too less , it will lead to wrinkled
appearance of the facial skin
69.
However , thisguide is a relatively
unreliable one ; therefore should be used
with caution or in combination with
other methods
70.
Whether the faceis appearing long or
otherwise is subjective
If the facial skin of the patient is already
wrinkled , one may be tempted to
increase the vertical dimension excessively
71.
SWALLOWING THRESHOLD
The positionof the mandible at the
beginning of the swallowing act has been
used as a guide establish the vertical
dimension of occlusion
When a person swallows, the teeth come
together with a very light contact at the
beginning of the swallowing
72.
If the dentureteeth fail to contact during
swallowing , the VDO is excessively
reduced
73.
TACTILE SENSATION
The patient’stactile sense can be used as a
guide to the determination of the VDO
The problem with this method relates to
presence of foreign objects in the palate &
the tongue space which can obscure the
patient's judgment
CENTRIC JAW RELATION
Therelationship of mandible to maxilla ,
when the mandible is in the most
posterior / retruded ,unstrained position
in relation to the maxilla, at an
established vertical dimension
WHAT DOES THIS STATEMENT
IMPLY ???
78.
“The Maxillomandibular relationshipin
which the condyles articulate with the
thinnest avascular portion of the articular
disc & the complex (of articular disc and
the head of condyle) braced
anterosuperiorly against the (posterior)
slopes of the articular eminence”
79.
When the naturalteeth are present, the
proprioceptive impulses from the teeth
guide the movement of the mandible so
the teeth can come in occlusion in a
comfortable position
80.
When the naturalteeth are absent, the
proprioceptive impulses from the the
Temporomandibular joint guide the
movement of the mandible so that the
mandible can close in a comfortable &
unstrained position
81.
It is atthis comfortable position , the
denture teeth should come in occlusion
with each otherc
The comfortable position is the Centric
Relation Position
The occlusion of the denture teeth in this
comfortable position is the Occlusion at
Centric Relation Position / Centric
Occlusion
82.
SIGNIFICANCE OF CENTRICRELATION
POSITION
•The recording of the Centric relation
position is the starting point for
developing occlusion in the complete
dentures
•It is a bone to bone relation
•It is a hinge position
83.
•It is anideal arch to arch relation and an
optimum functional position of the jaws
for the health, comfort & function of the
TMJ and musculature
•During swallowing the mandible is at
/near the centric relation position
•It is a learnable , repeatable &
reproducible position
84.
Although the positionis reproducible , it
is difficult to record it with sufficient
accuracy in edentulous patients
BIOLOGICAL
DIFFICULTIES
PSYCHOLOGIC
DIFFICULTIES
MECHANICAL
DIFFICULTIES
85.
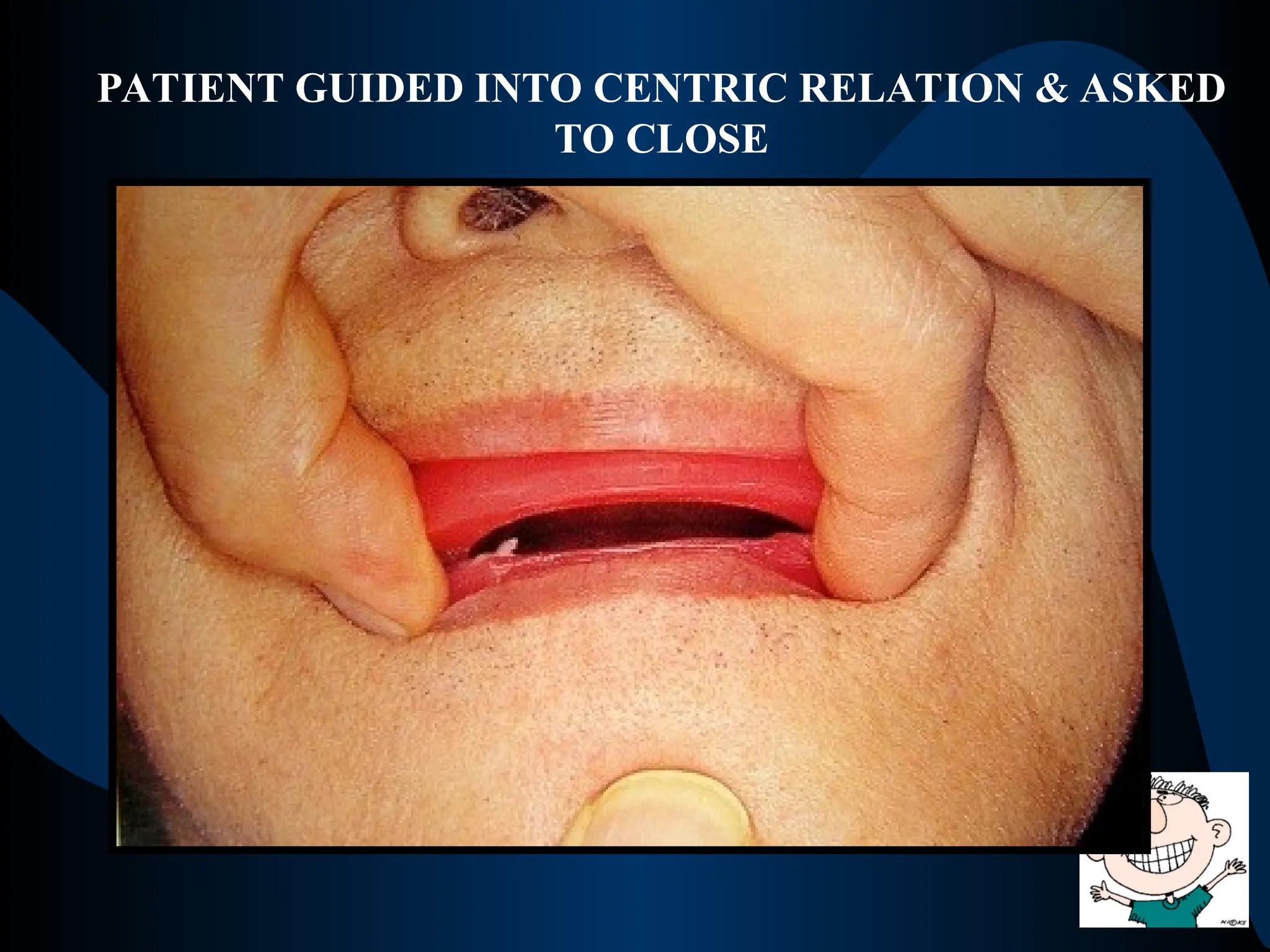
Instructions can begiven to assist patient
to retrude the mandible
“Let your jaw relax , pull it back ,and close
slowly and easily on your back teeth”
“Get the feeling of pushing your upper jaw
out & closing your back teeth together”
86.
Instruct the patientturn the tongue
backwards towards the posterior part of the
hard palate
Instruct the patient to protrude & retrude the
mandible repeatedly while holding his or her
fingers lightly against the chin
87.
METHODS TO RECORDTHE
CENTRIC JAW RELATIONS
Interocclusal
Check records
Wax Squash
Bite
Pressure – less
method
STATIC METHODS
88.
Can be madeat the stage of Try- in of the
waxed up trial dentures after the arrangement
of teeth
INTEROCCLUSAL CHECK RECORDS
89.
A softened sheetof Aluwax is placed between
the upper & lower teeth on the trial dentures
The patient is guided into centric relation
position
The patient is then asked to close in that
position without contacting the teeth
90.
WAX SQUASH BITE
Involvesplacement of a horse-shoe shaped
roll of softened wax between maxillary &
mandibular rims and having the patient close
the jaws in centric relation
91.
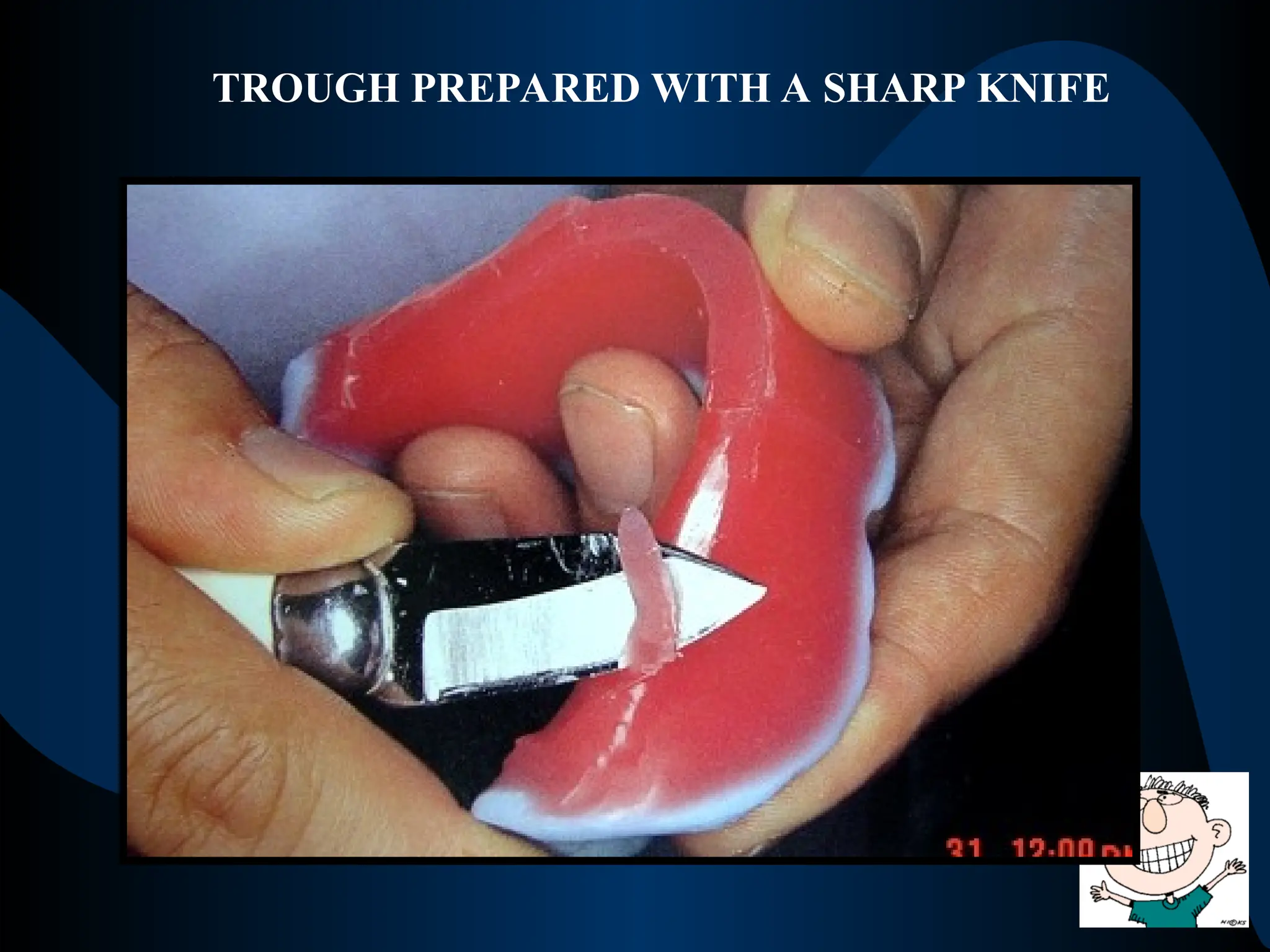
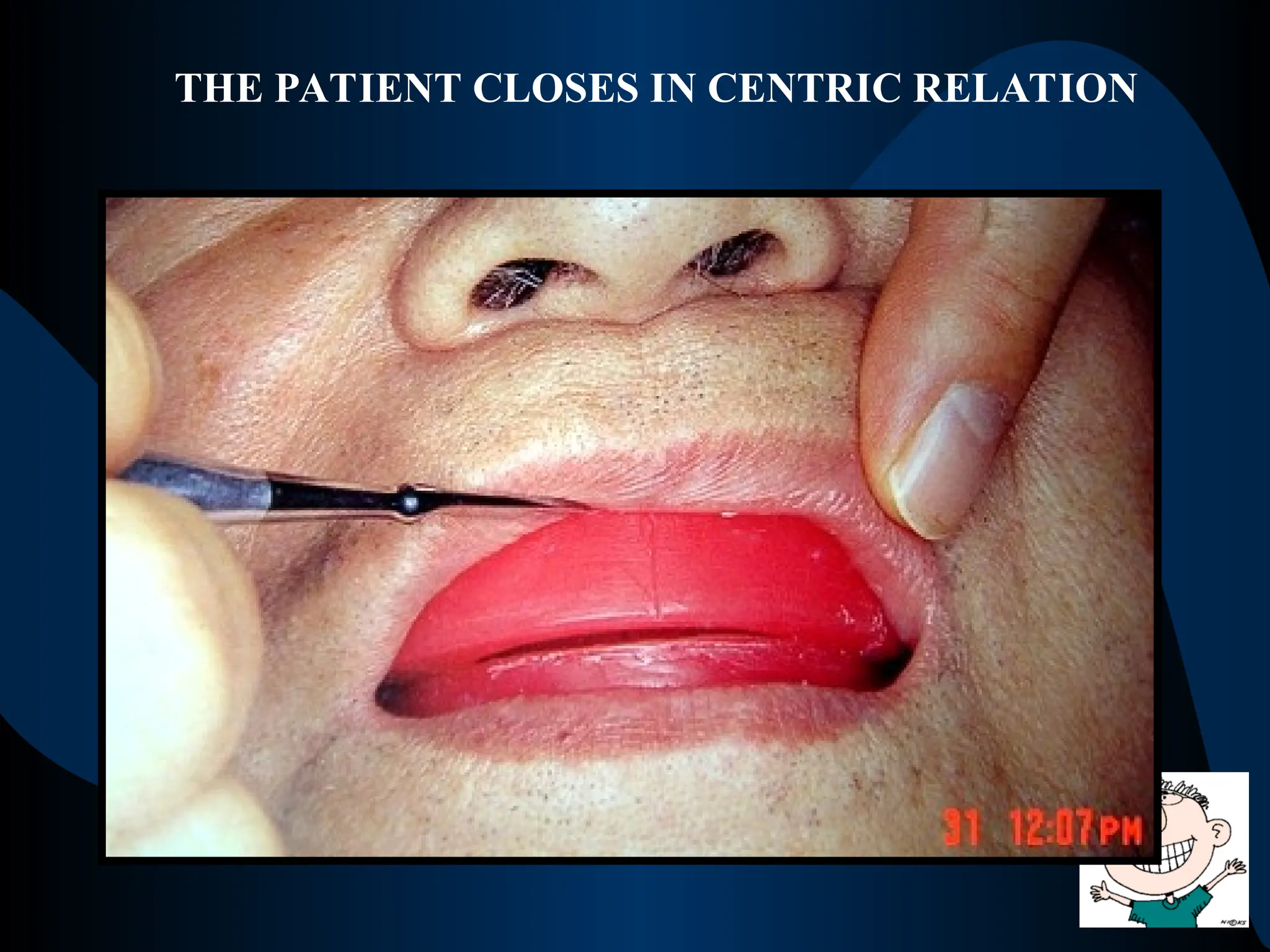
PRESSURE - LESSMETHOD
The occlusal rims are adjusted to establish the
correct vertical dimension
The patient is trained to close in centric
relation position
The wax can then be sealed in centric relation
position using Nick & Notch method / Staple
pins
92.
These methods usefunctional movements of
the jaw to record the centric relation
The patient is asked to perform lateral and
protrusive movements in order to identify the
centric relation position of the mandible
NEEDLE HOUSE
TECHNIQUE
PATTERSON’S
TECHNIQUE
FUNCTIONAL METHODS
93.
These methods arecalled so because they
use graphs / tracings to record various jaw
movements & centric jaw relation position
Done with the help of tracing apparatus
2 types of tracings
ARROW POINT TRACING PANTOGRAPHIC TRACING
One dimensional tracing Three dimensional tracing
GRAPHIC METHODS
94.
RADIOGRAPHIC METHODS
Lateral cephalometricradiograph can be used
to record the centric relation position by
studying the position of the condyles in relation
to the articular eminence
95.
ECCENTRIC JAW RELATION
Anyrelationship of the mandible to the
maxilla other than centric relation
It includes the recording of protrusive
and lateral movements of the mandible
The basic purpose is to be able to
reproduce these movements on the
articulator
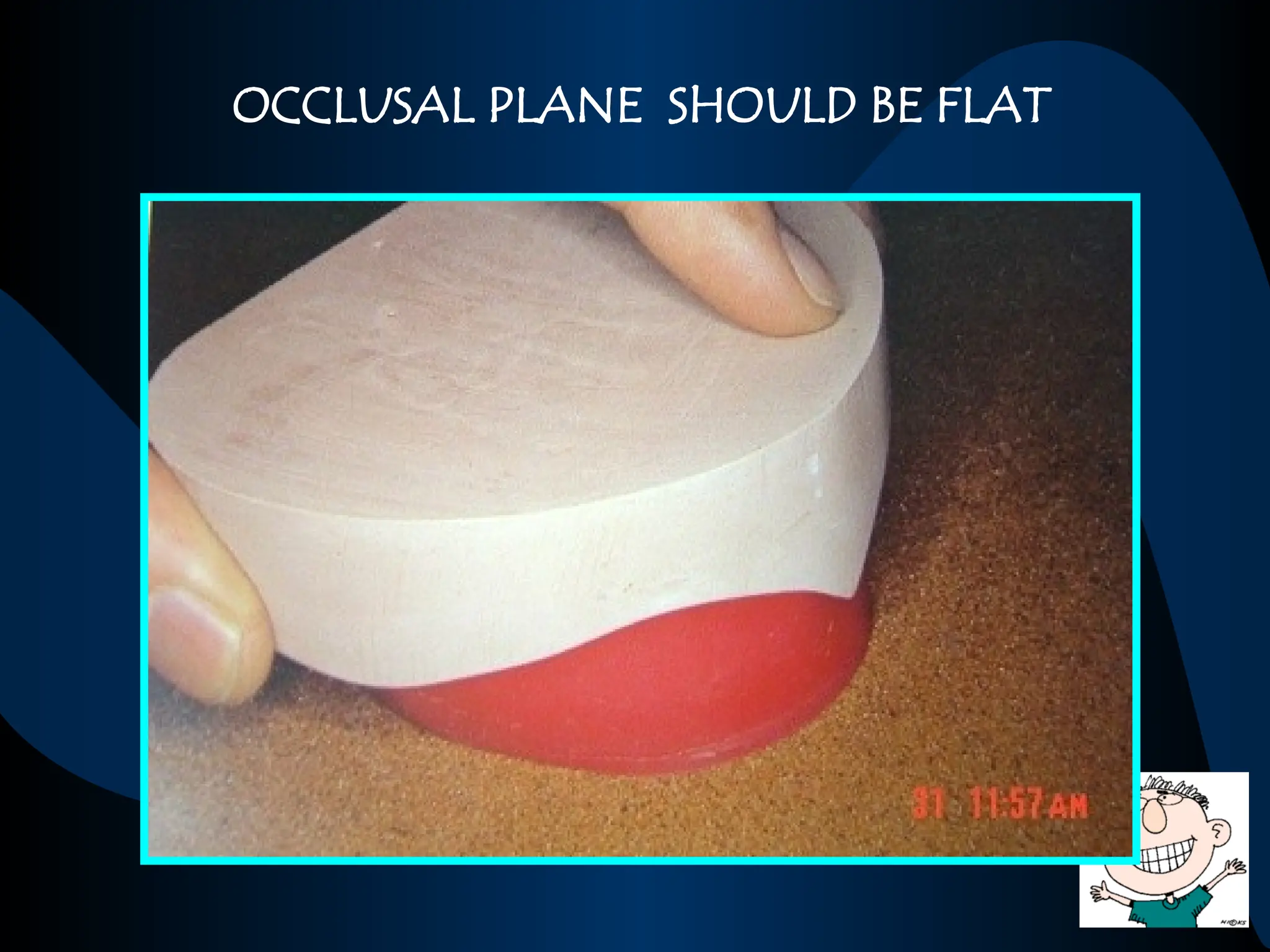
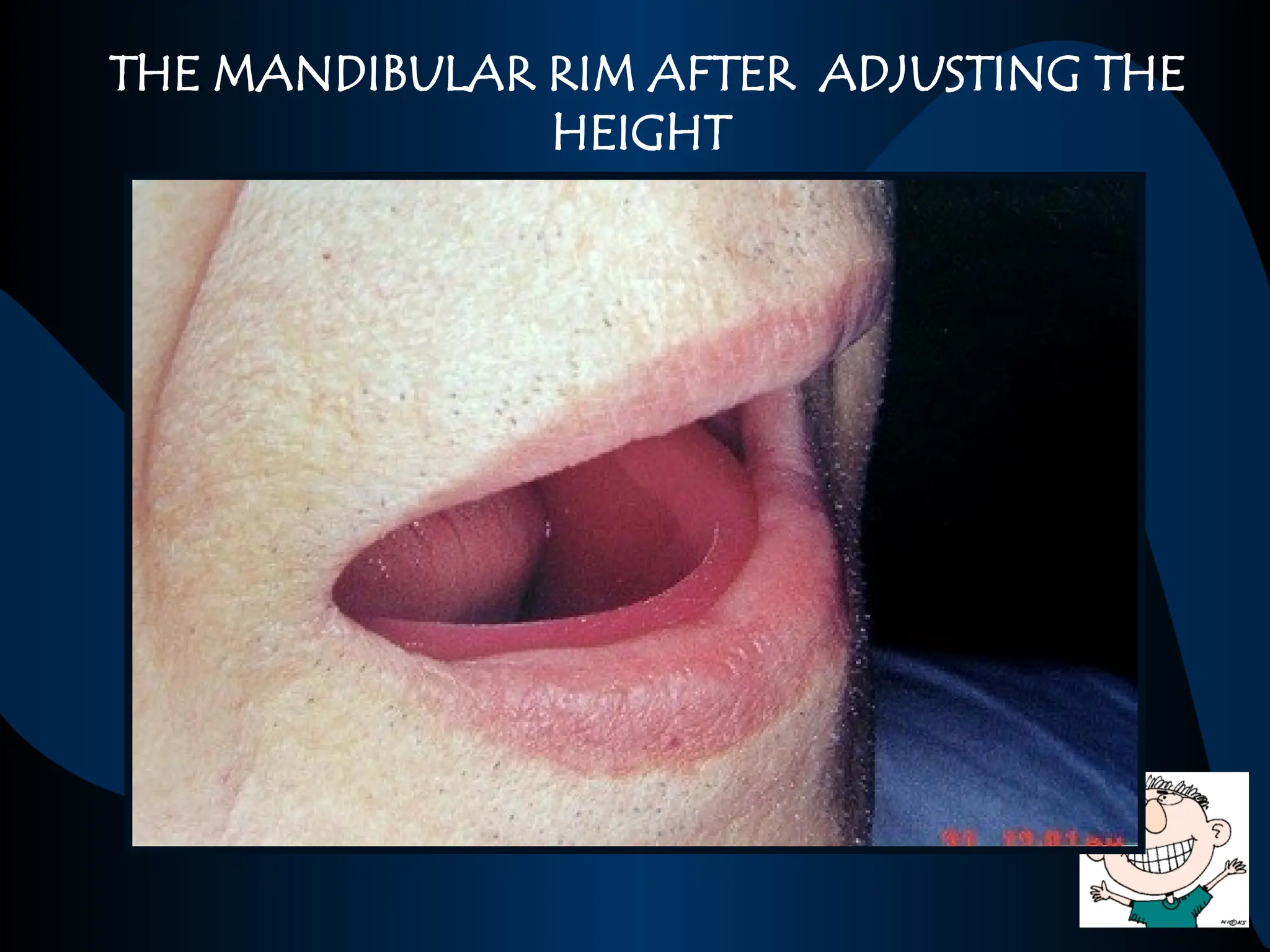
Once the occlusalplane of maxillary rim is
adjusted corrected, YOU SHOULD NOT
TOUCH THE PLANE AGAIN !!!
The vertical dimension is established by
adjusting the height of the mandibular wax
rim
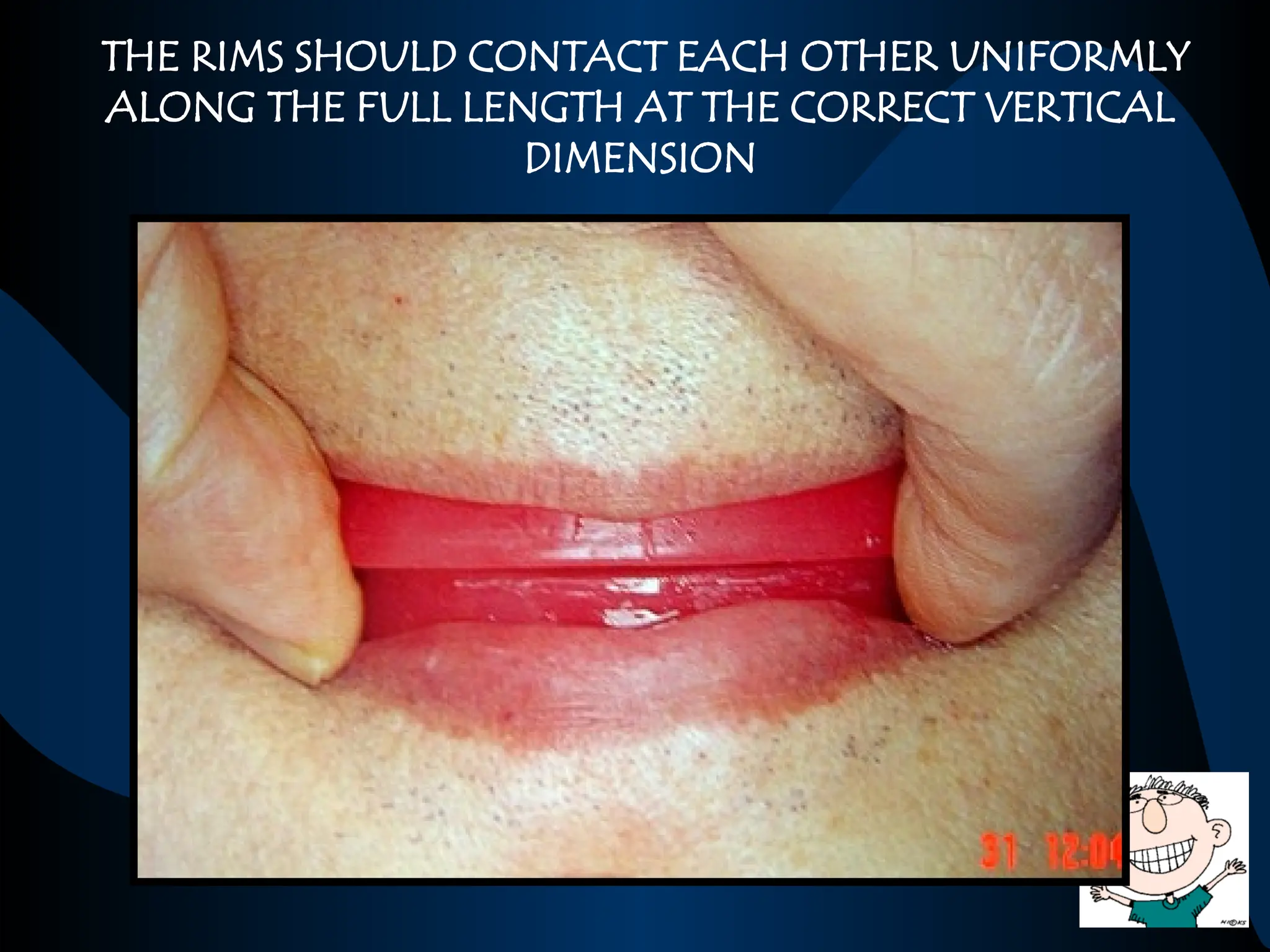
The patient isasked to swallow
Relax his lips and cheeks muscles
Lightly contact the lips
The lips are then parted to evaluate the
freeway space
HOW TO CHECK FOR THE CORRECTNESS OF THE
VERTICAL DIMENSION
I.
110.
The patient canbe asked to pronounce
words with sounds of ‘M’ instead of
swallowing action and the same procedure
can be repeated
Pronunciation of sibilants (words with
sounds of ‘S’) with clarity can also be used to
evaluate the correctness of VD
II.
111.
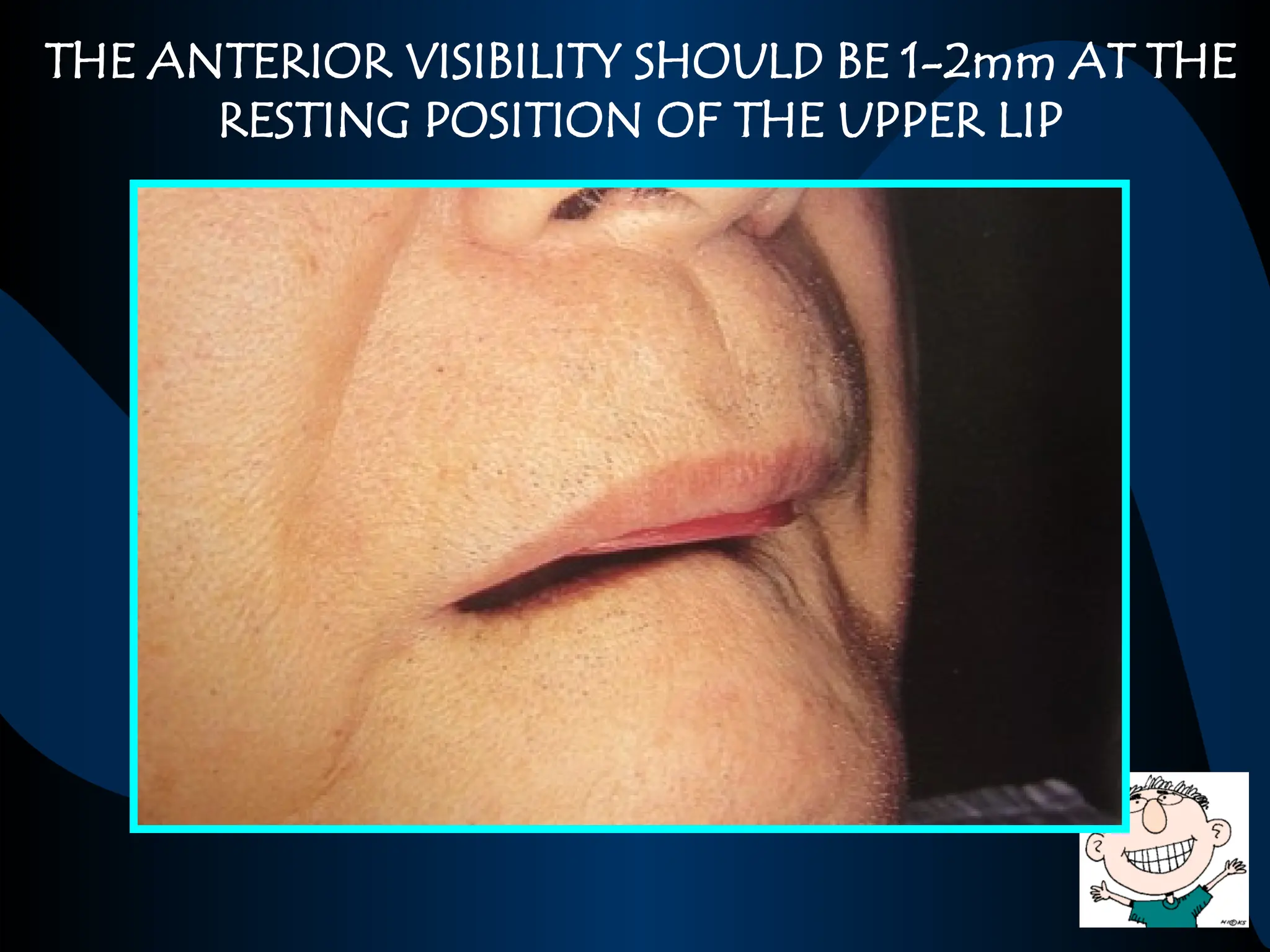
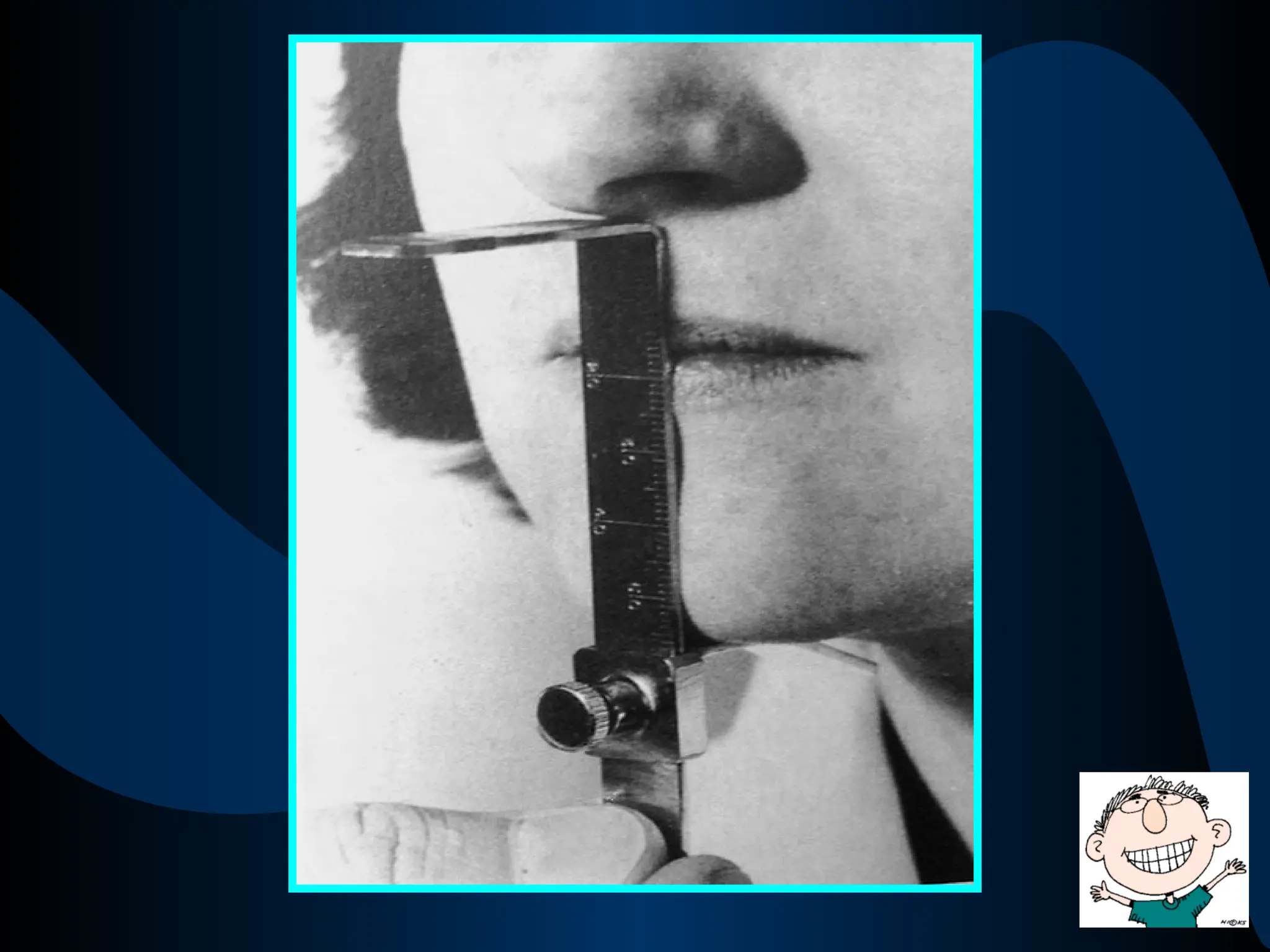
The distance betweenthe most prominent
point on the nose and the most prominent
point on the chin at rest and in occlusion can
be measured and the difference can be
calculated to evaluate the freeway space
e.g., VDR - 65 mm
VDO - 62 mm
VDR – VDO = FREEWAY SPACE=3mm
III.
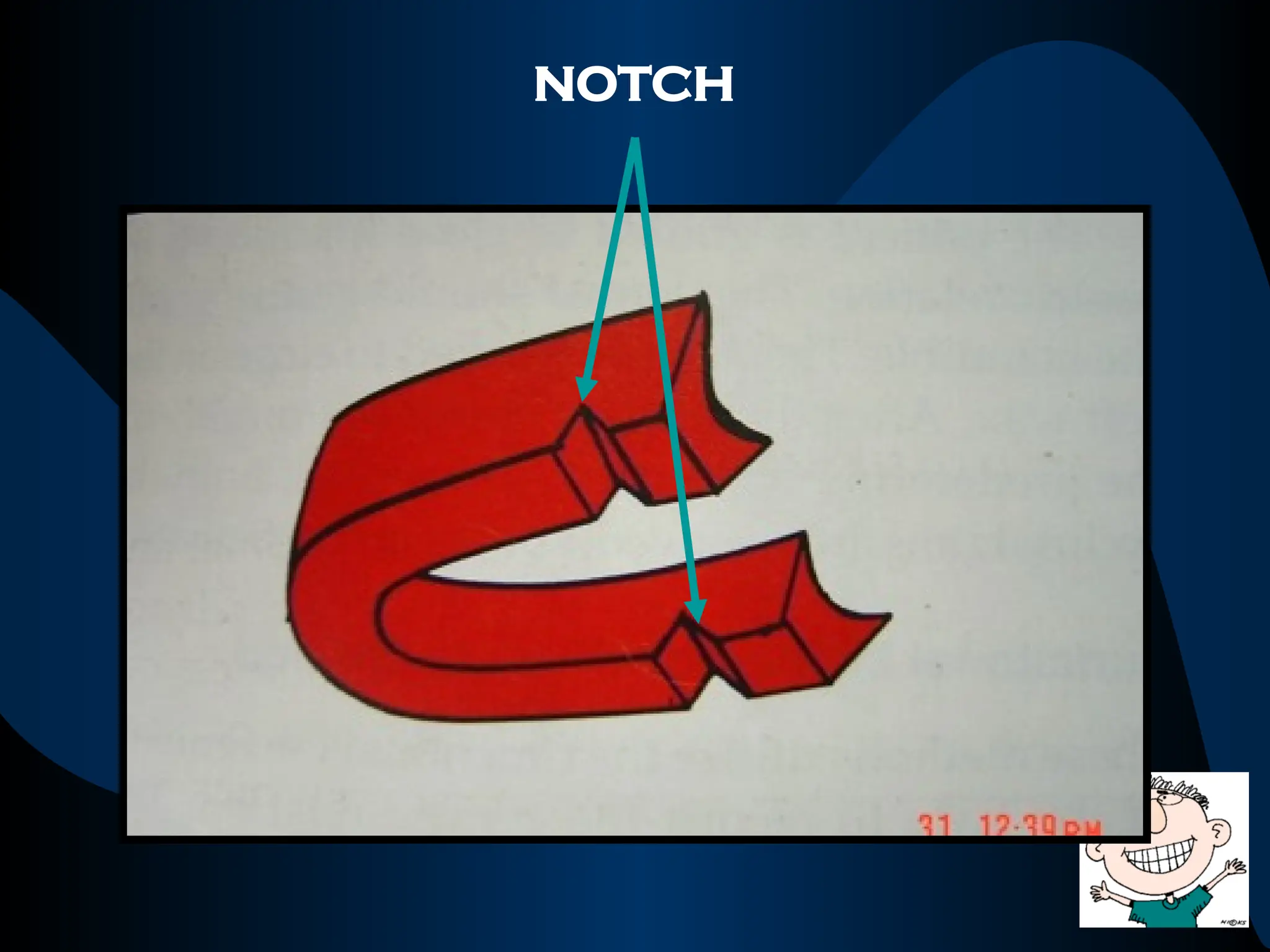
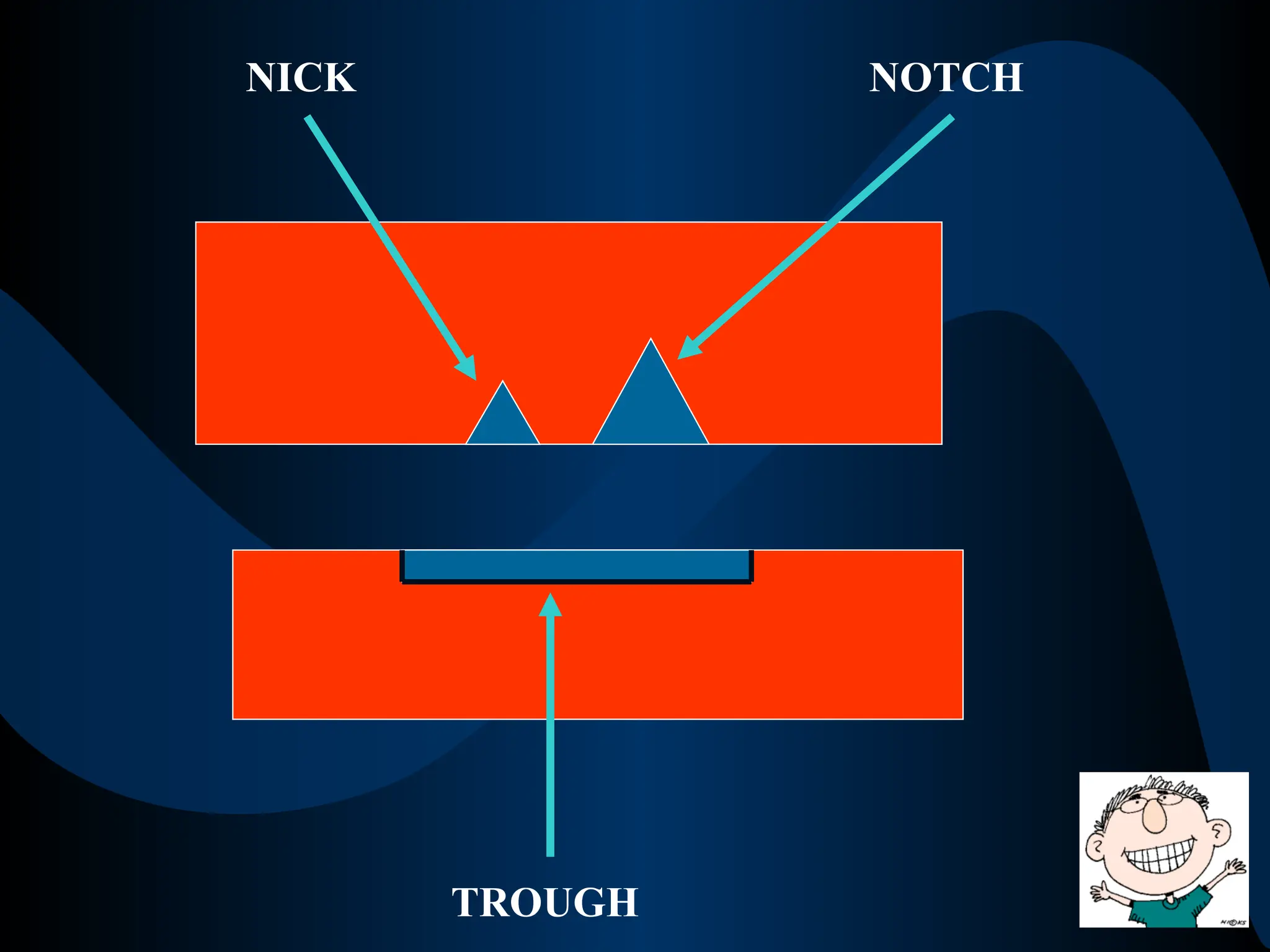
‘V’ shaped spacecreated on the maxillary
rim in the 1st
molar region crossing the full
width of the rim
Function : to prevent Anteroposterior
movement / sliding during centric relation
recording
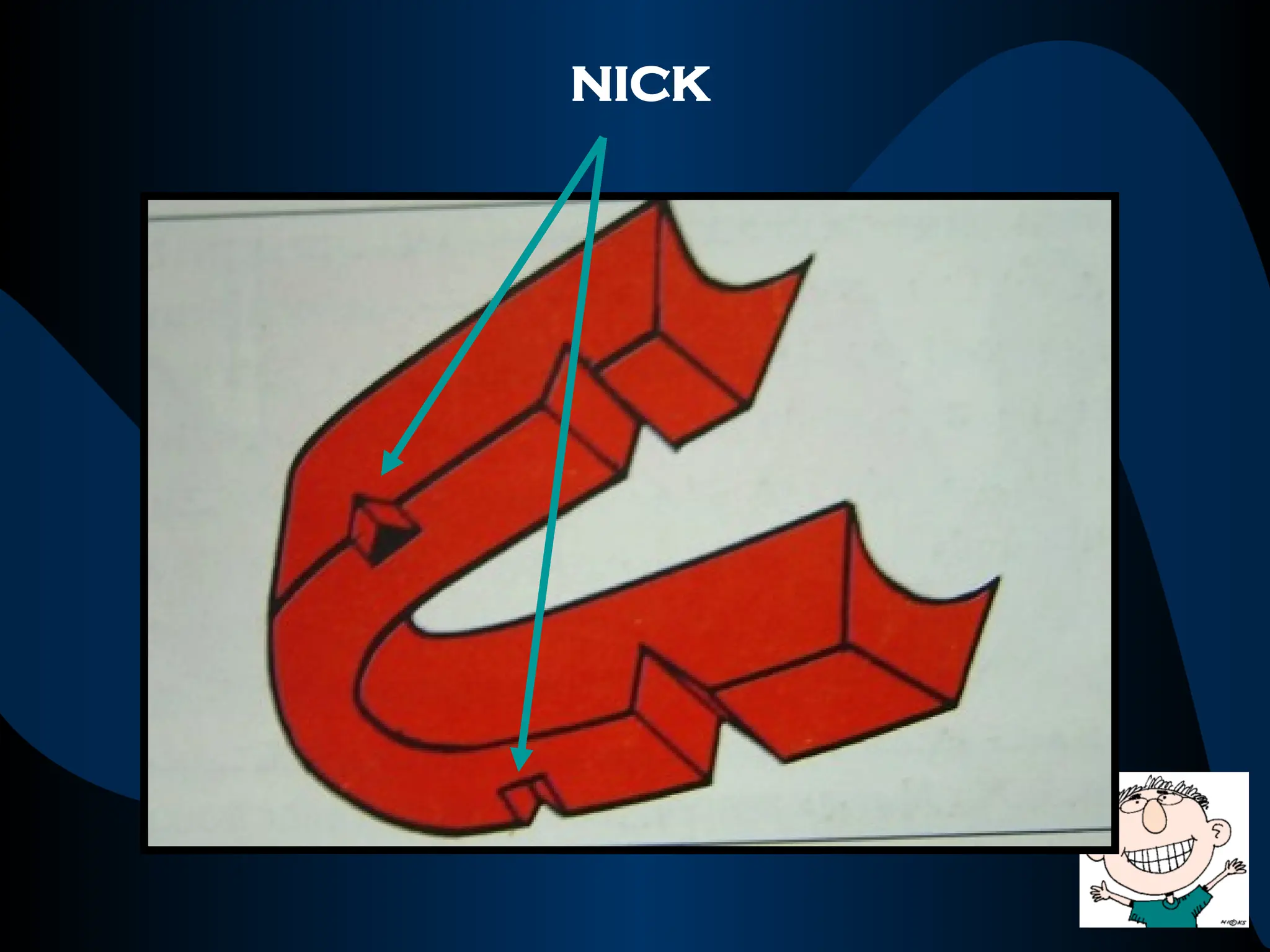
‘V’ shaped spacecreated on the maxillary
rim in the 2nd
premolar region not crossing
the full width of the rim
FUNCTION : to prevent Lateral movement /
sliding during centric relation recording
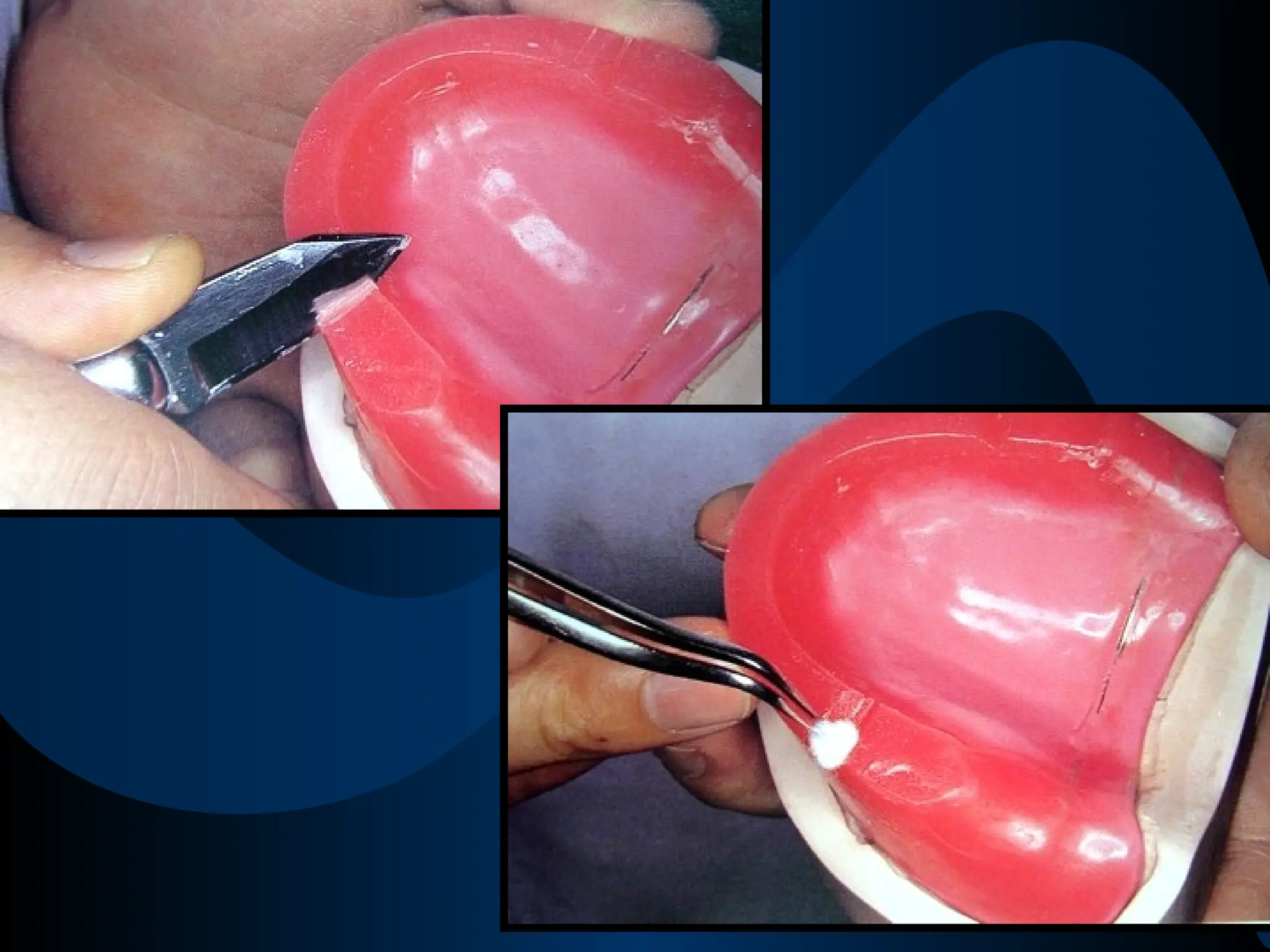
An area ofdepression created on the
mandibular rim in direct apposition to the
nick & notch on the maxillary rim
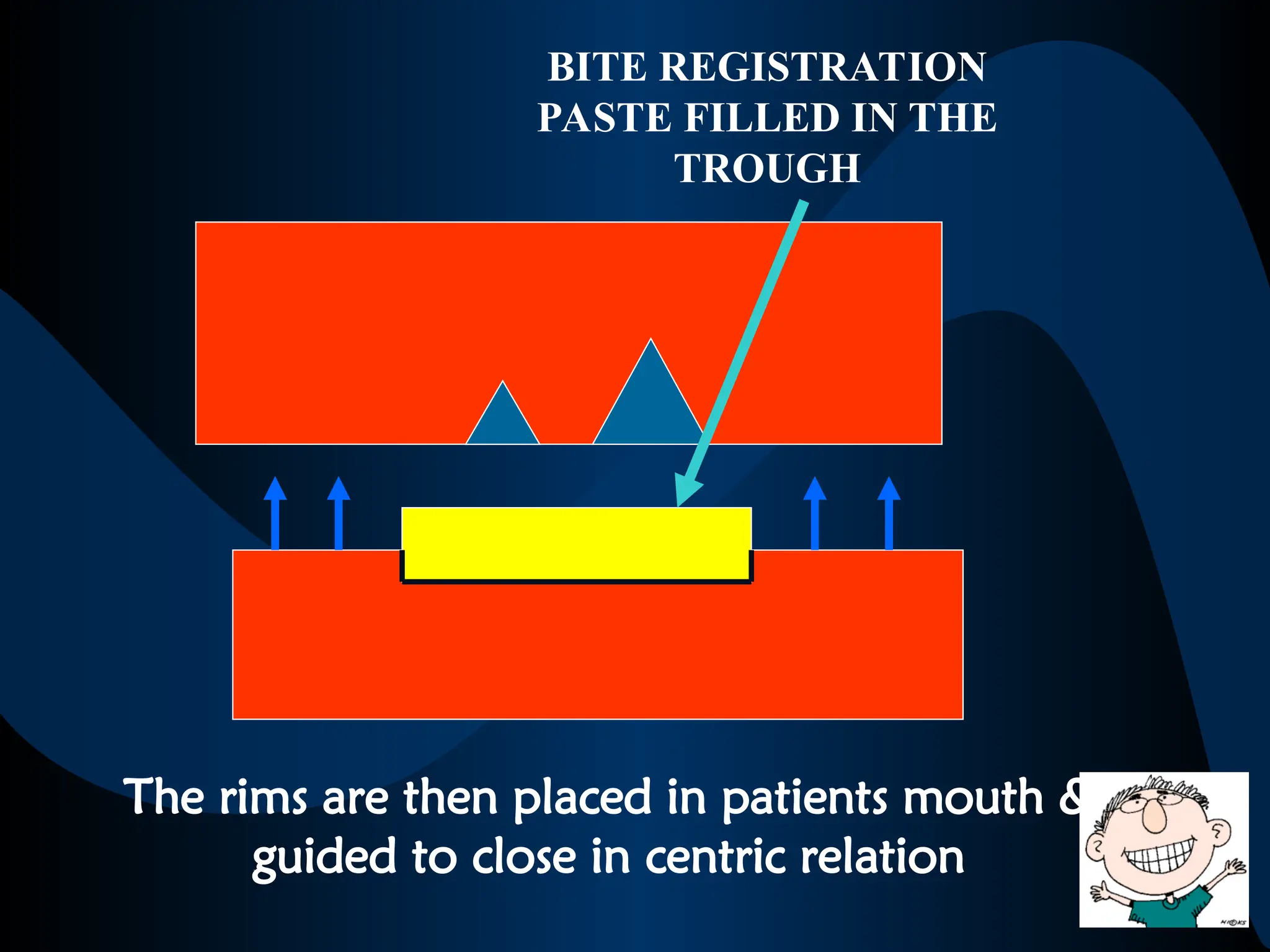
FUNCTION: to provide space for the bite
registration paste that will enter the nick and
notch













![Vertical Dimension of Rest (VDR)
“The amount of separation of the jaws
when the mandible is in a
Physiologic Rest Position”
It is the position where the muscles that close
the jaws and those that open the jaws are in a
state of minimal contraction [function], just
enough to maintain the posture of mandible](https://image.slidesharecdn.com/jawrelations-250530172359-28b17a76/75/JAW-RELATIONS-ppt-40-2048.jpg)



































![vertical jaw relation [Autosaved].pptx .](https://cdn.slidesharecdn.com/ss_thumbnails/verticaljawrelationautosaved-250920192706-cb5ca831-thumbnail.jpg?width=640&height=640&fit=bounds)















































