Download to read offline

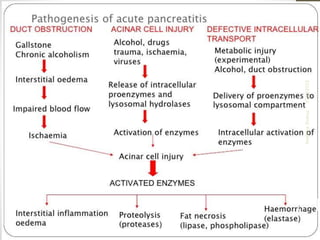
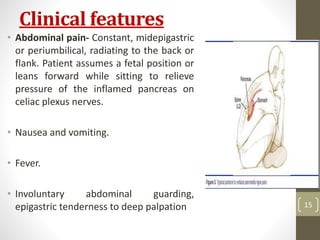

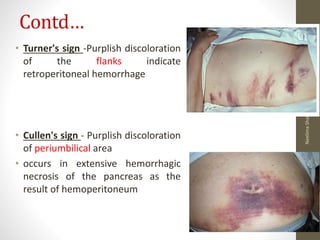
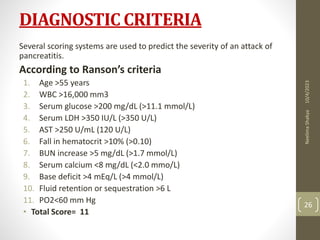
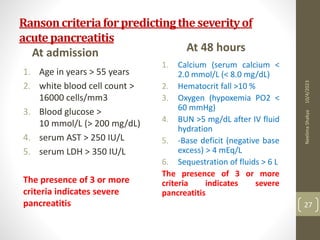


This document provides an overview of pancreatitis including: - Defining pancreatitis and describing the types as acute or chronic. - Stating the common causes as biliary disease, alcohol, ERCP, trauma, and drugs. - Explaining the pathophysiology as premature activation of digestive enzymes in the pancreas causing autodigestion. - Identifying clinical manifestations such as abdominal pain, nausea, fever, and diagnostic tests including blood tests and imaging. - Describing the management of fluid resuscitation, pain control, nutritional support, and antibiotics as well as surgical interventions for complications.