Downloaded 31 times









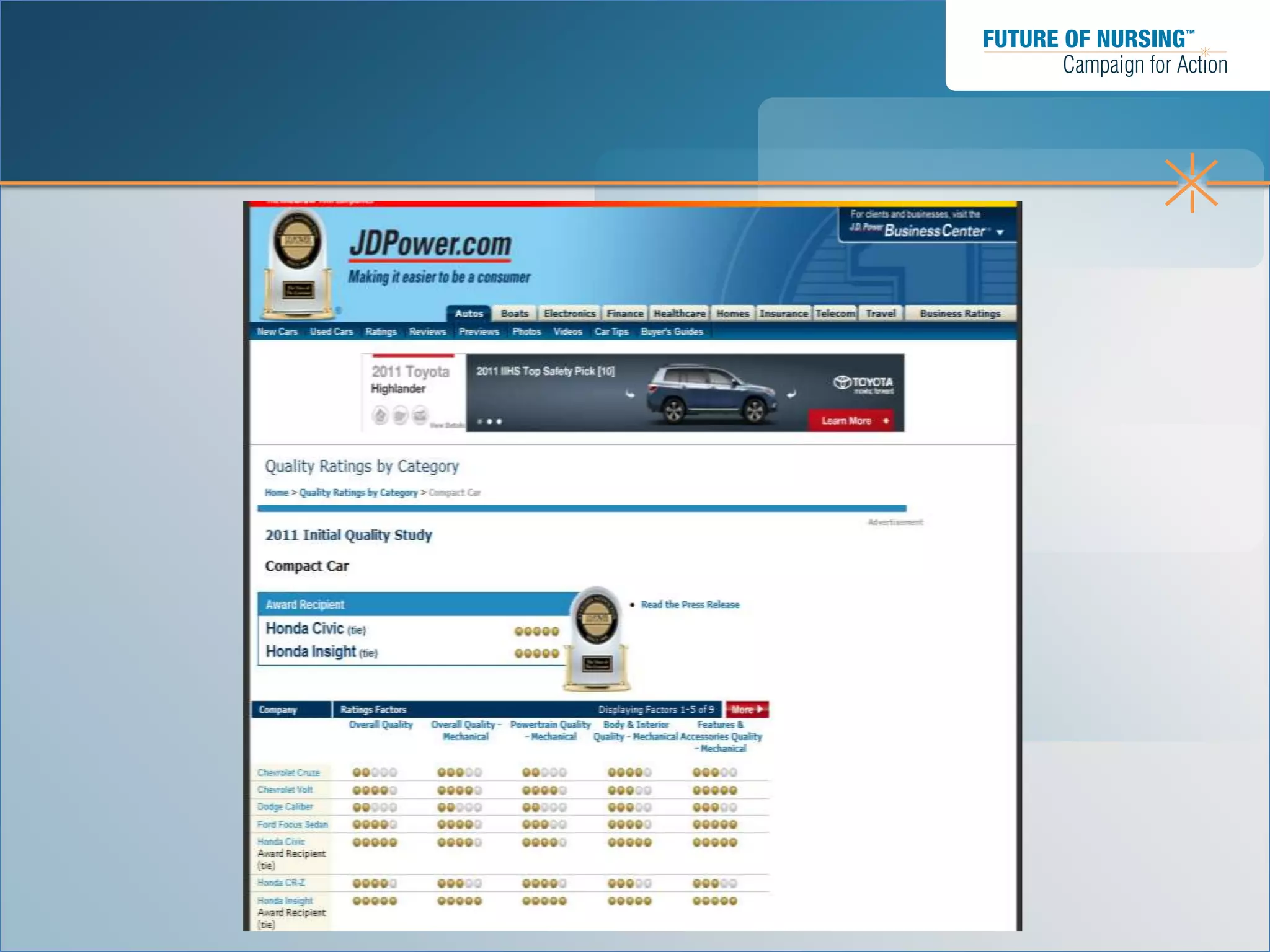
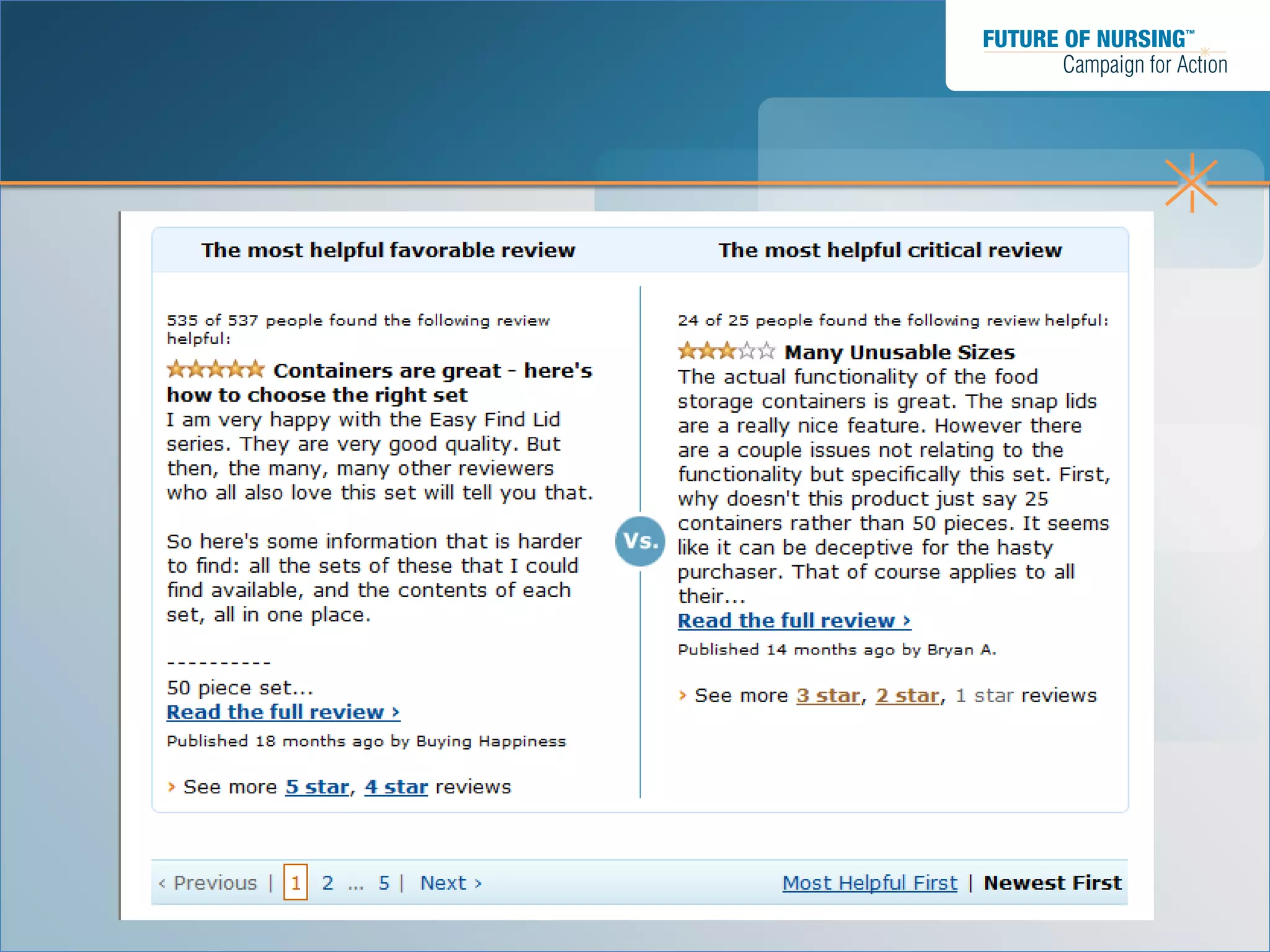
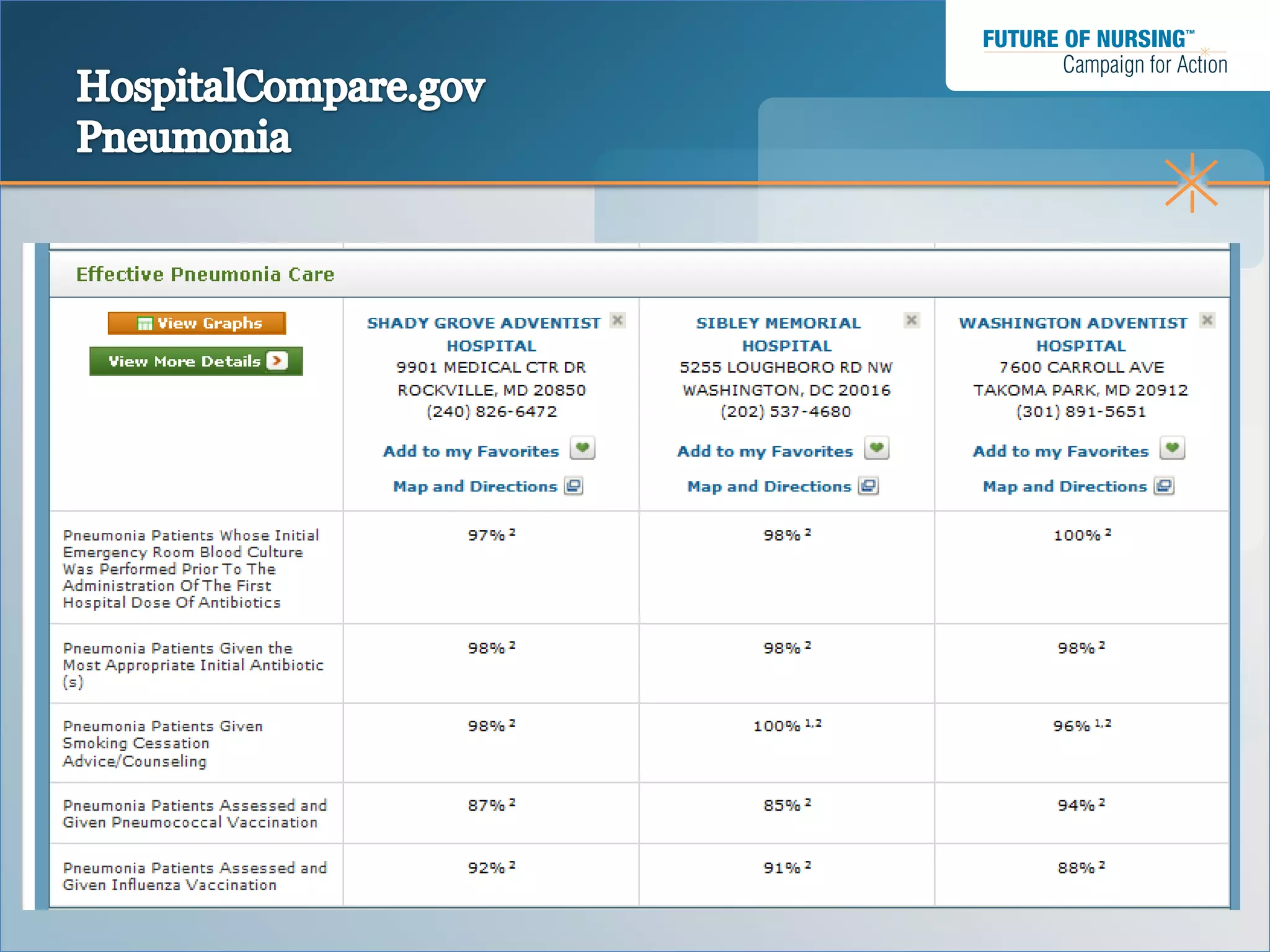
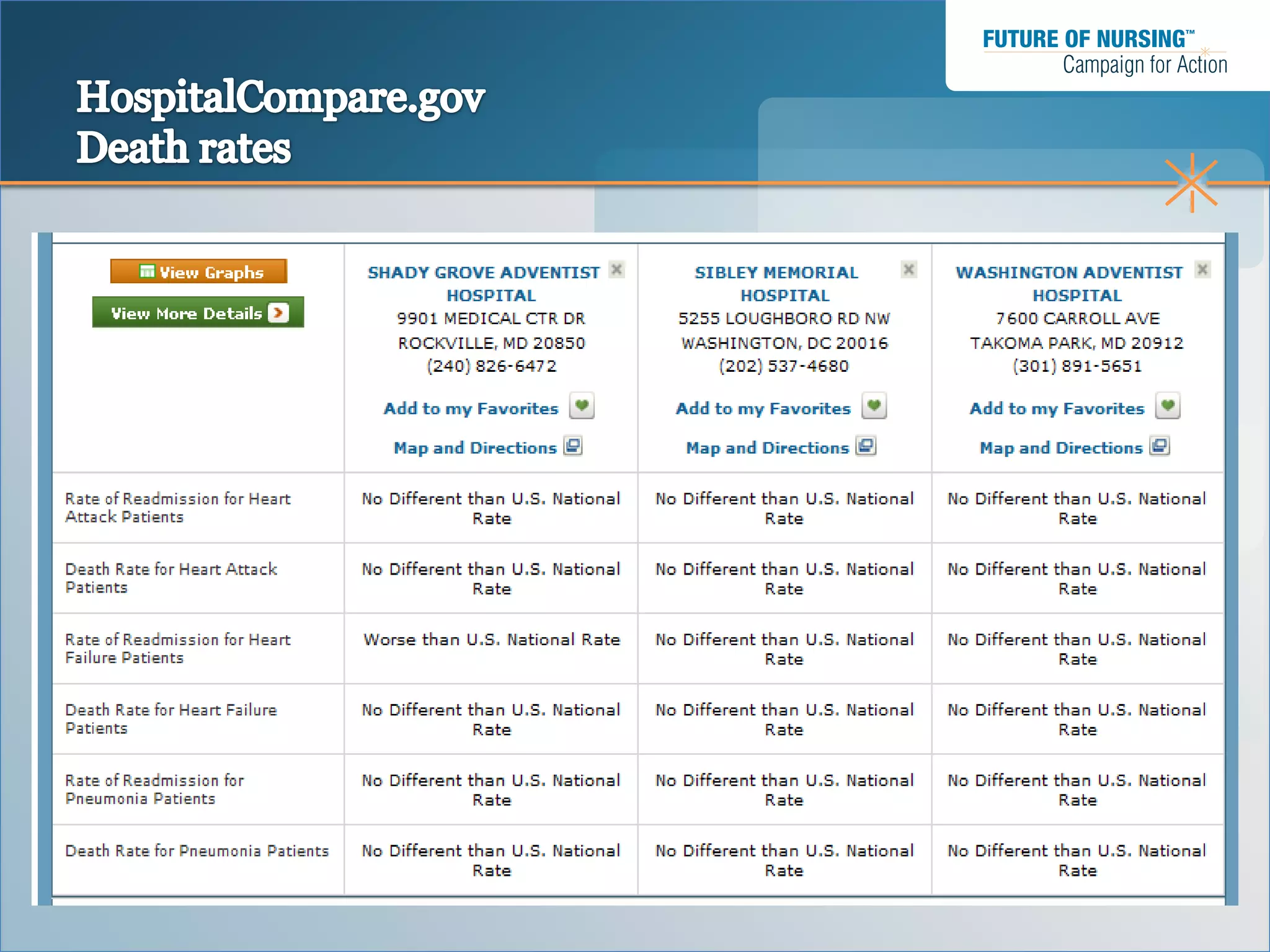


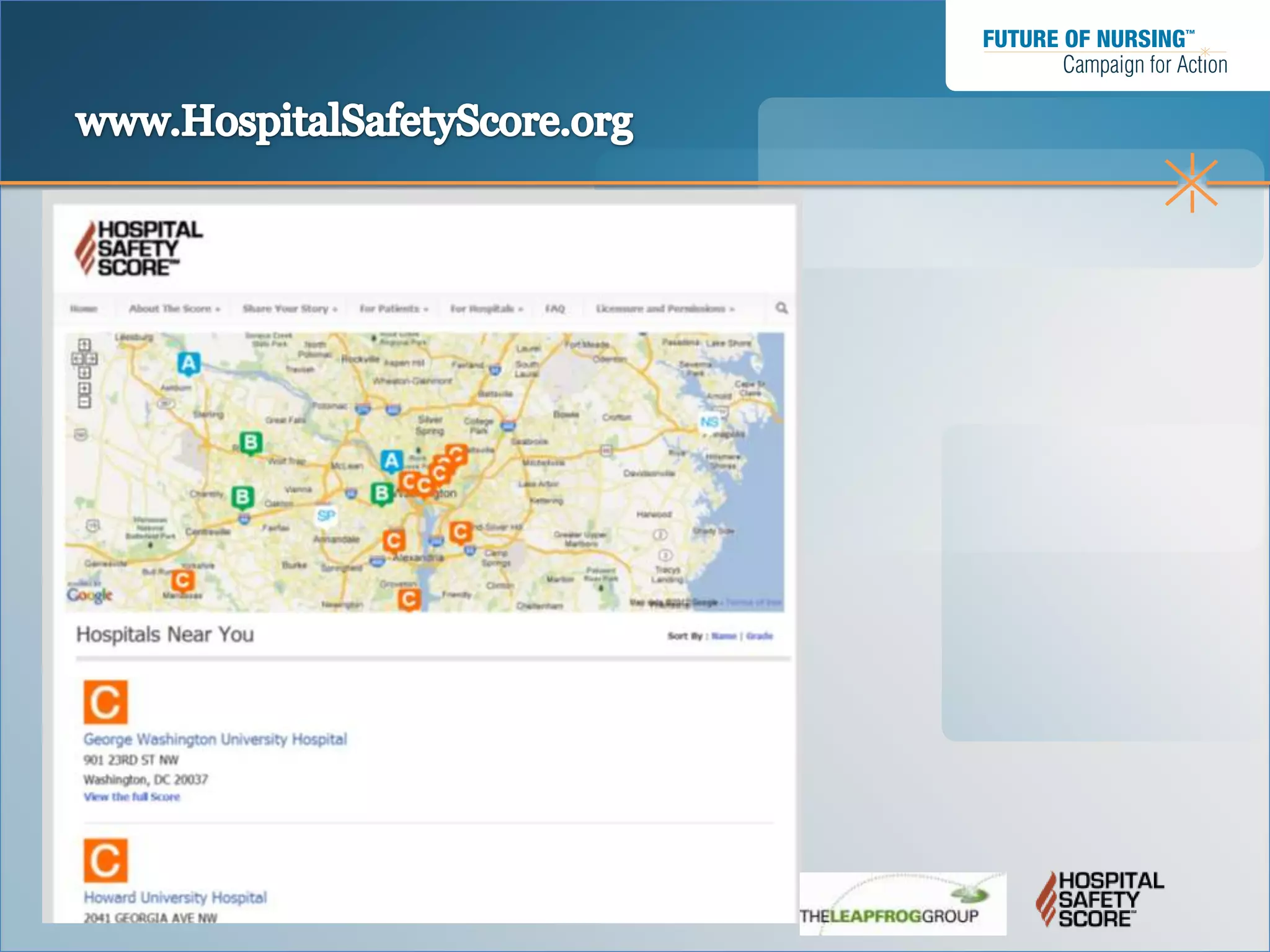
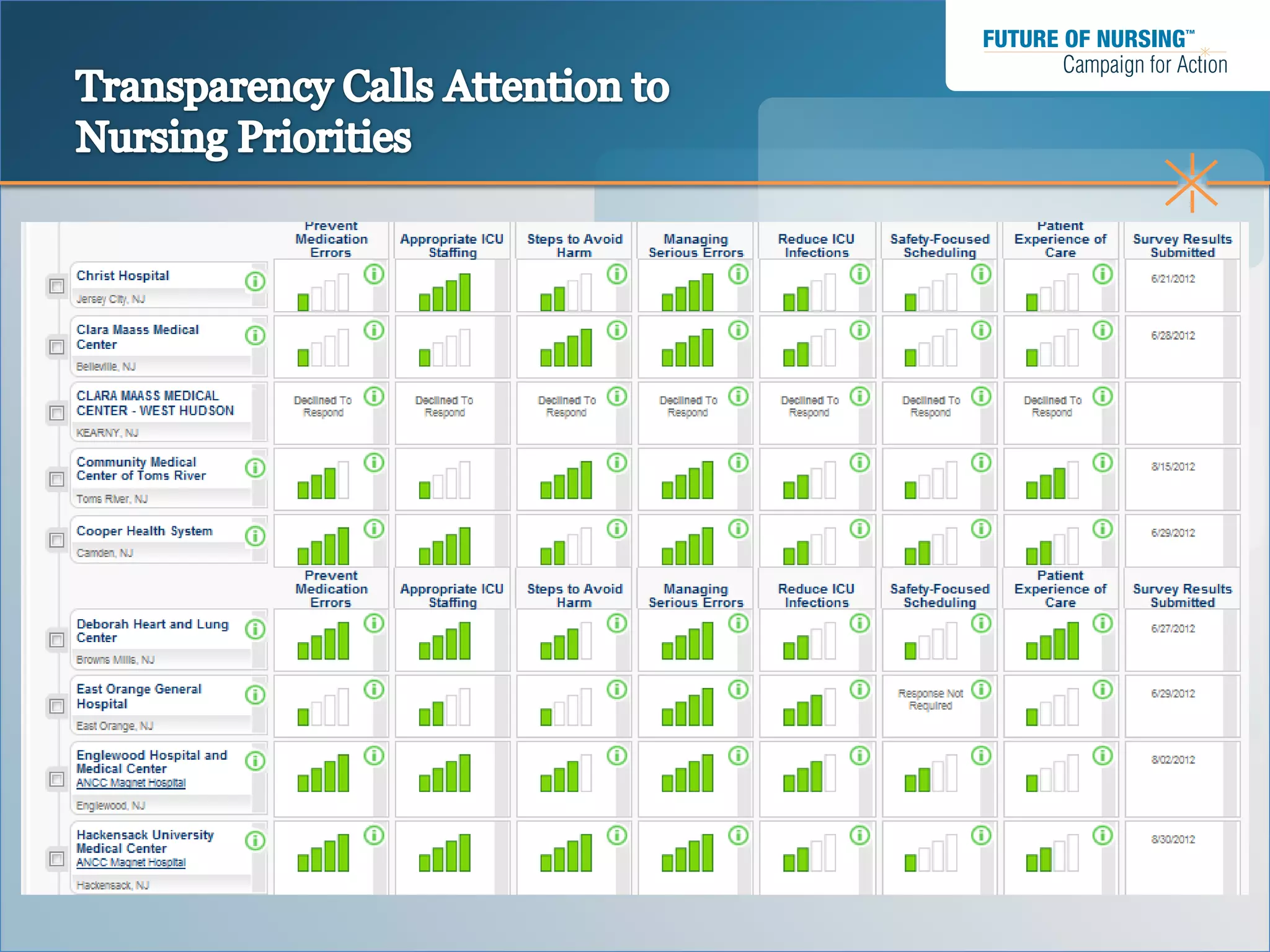


The document summarizes a webinar presented by The Leapfrog Group on hospital safety. The webinar discusses Leapfrog's role in publicly reporting hospital safety scores and ensuring a prepared nursing workforce. Leapfrog develops the Hospital Safety Score - a letter grade reflecting how well hospitals prevent errors and harm - using national data. Experts provide guidance on calculating the scores. The scores aim to show hospital performance variation, be relevant to consumers, and report data independently. Magnet status recognition considers nursing factors important to safety.





















![Role of infection control in patient safety [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/roleofinfectioncontrolinpatientsafetycompatibilitymode-131231012445-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


























![Roshni Bag Thesis [PDF]](https://cdn.slidesharecdn.com/ss_thumbnails/be88bc60-4627-46a6-a858-f9935eb861dd-170103024230-thumbnail.jpg?width=640&height=640&fit=bounds)














































