Downloaded 757 times


![ Safety culture
A culture that exhibits the following five high-level
attributes that health care professionals strive to
operationalize through the implementation of strong
safety management systems.
(1) A culture where all workers (including front-line staff, physicians, and
administrators) accept responsibility or the safety of themselves, their
coworkers, patients, and visitors.
(2) [A culture that] prioritizes safety above financial and operational goals.
(3) [A culture that] encourages and rewards the identification, communication, and
resolution of safety issues.
(4) [A culture that] provides for organizational learning from accidents.
(5) [A culture that] provides appropriate resources, structure, and accountability to
maintain effective safety systems.](https://image.slidesharecdn.com/patientsafety-120221041254-phpapp02/85/Patient-safety-31-320.jpg)

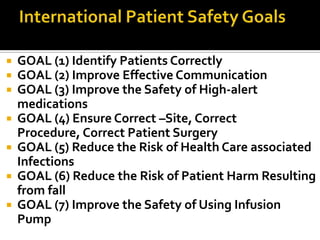
Patient safety aims to prevent harm caused by healthcare itself. While most medical care is delivered safely, errors still occur and patient safety has increasingly been recognized as an important global issue, though more work is needed to address it. Common causes of harm include individual errors, system issues, and environmental factors, and strategies like checklists and protocols seek to improve safety.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












