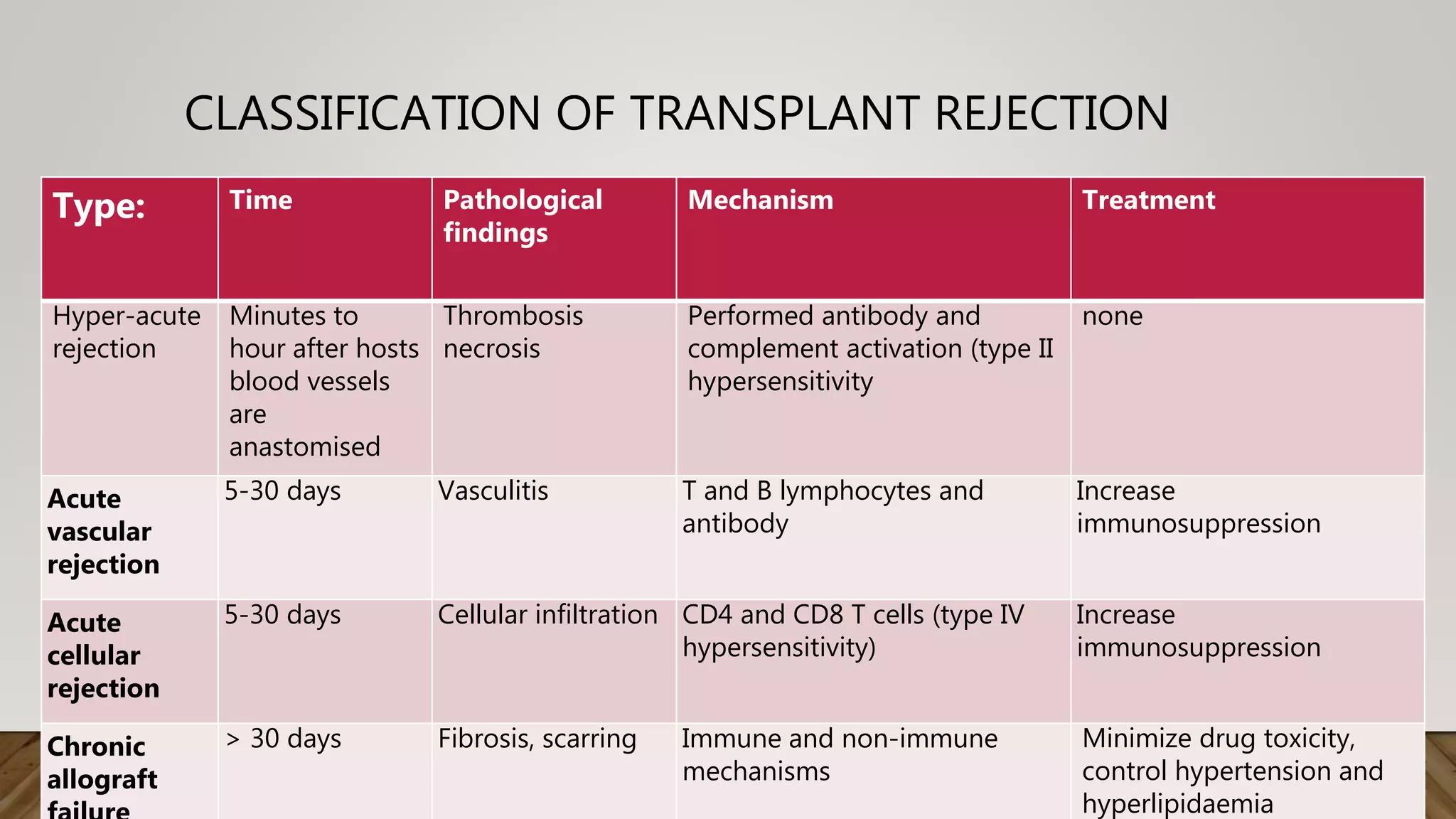
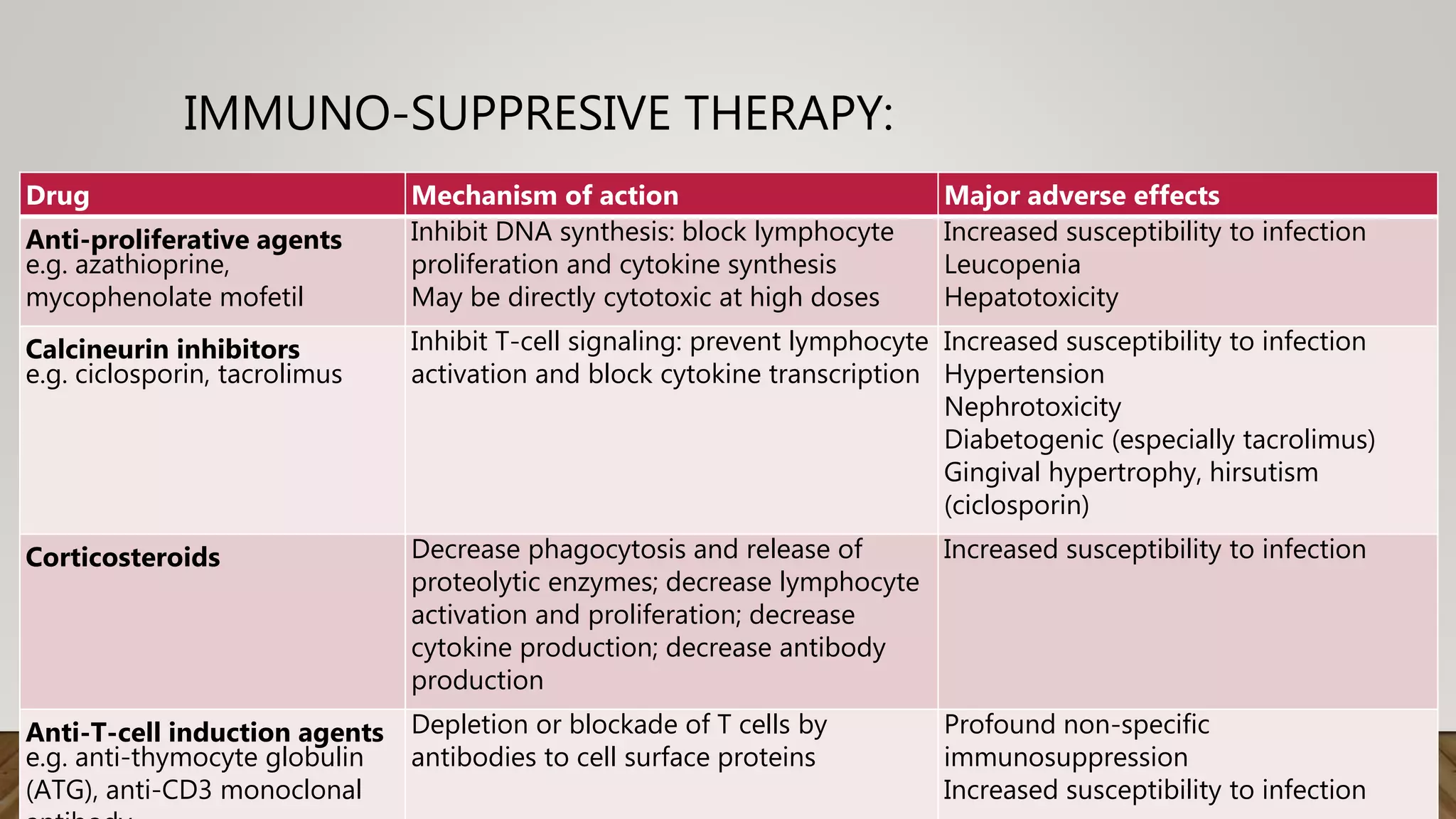
Organ transplantation involves transferring a whole or partial organ from a donor to a recipient in need of replacement of a damaged or failing organ. Major transplantable organs include the liver, kidney, heart, lungs, pancreas and intestine. Transplant rejection is a major complication that occurs when the recipient's immune system attacks the donor organ. The main types of rejection are hyperacute, acute vascular, acute cellular and chronic rejection. Rejection is combatted using immunosuppressive drugs that inhibit lymphocyte proliferation and activation such as corticosteroids, calcineurin inhibitors, antiproliferatives and anti-T cell agents. With advances in immunosuppression and organ matching, transplantation has become an established treatment for end-stage organ

















![Transplant immunology edd[1]](https://cdn.slidesharecdn.com/ss_thumbnails/transplantimmunologyedd1-190111094555-thumbnail.jpg?width=640&height=640&fit=bounds)
































































