Downloaded 1,412 times
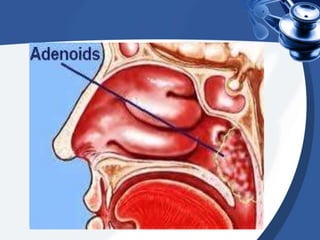
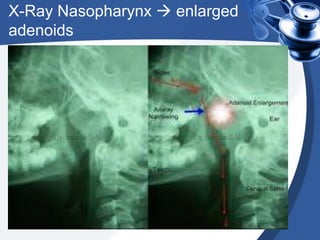

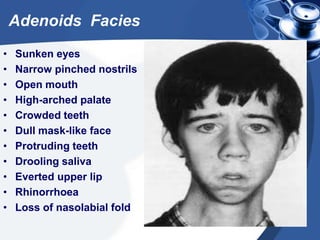


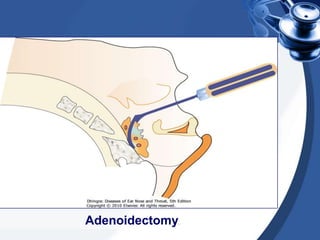
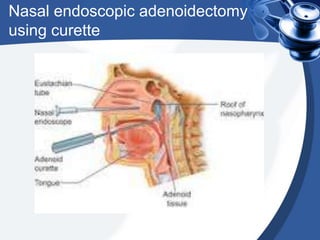
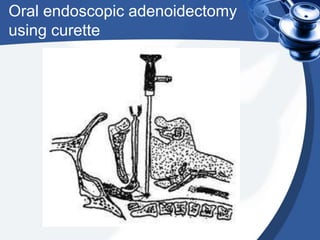


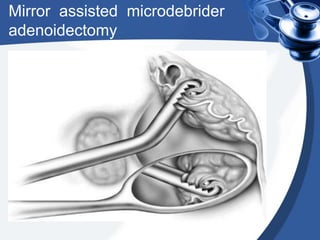
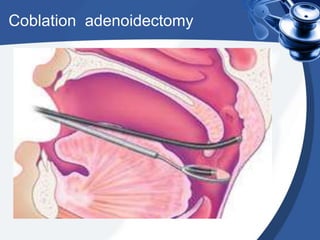


Adenoids are masses of lymphatic tissue located in the nasopharynx that can become enlarged. Symptoms of enlarged adenoids include nasal obstruction, mouth breathing, and ear infections. Adenoidectomy is the surgical removal of the adenoids and indications include recurrent infections and airway obstruction. The procedure involves using curettes or microdebriders to gently remove the adenoids under anesthesia. Post-operative care focuses on pain management, antibiotics, and monitoring for potential complications like bleeding or injury.



































































