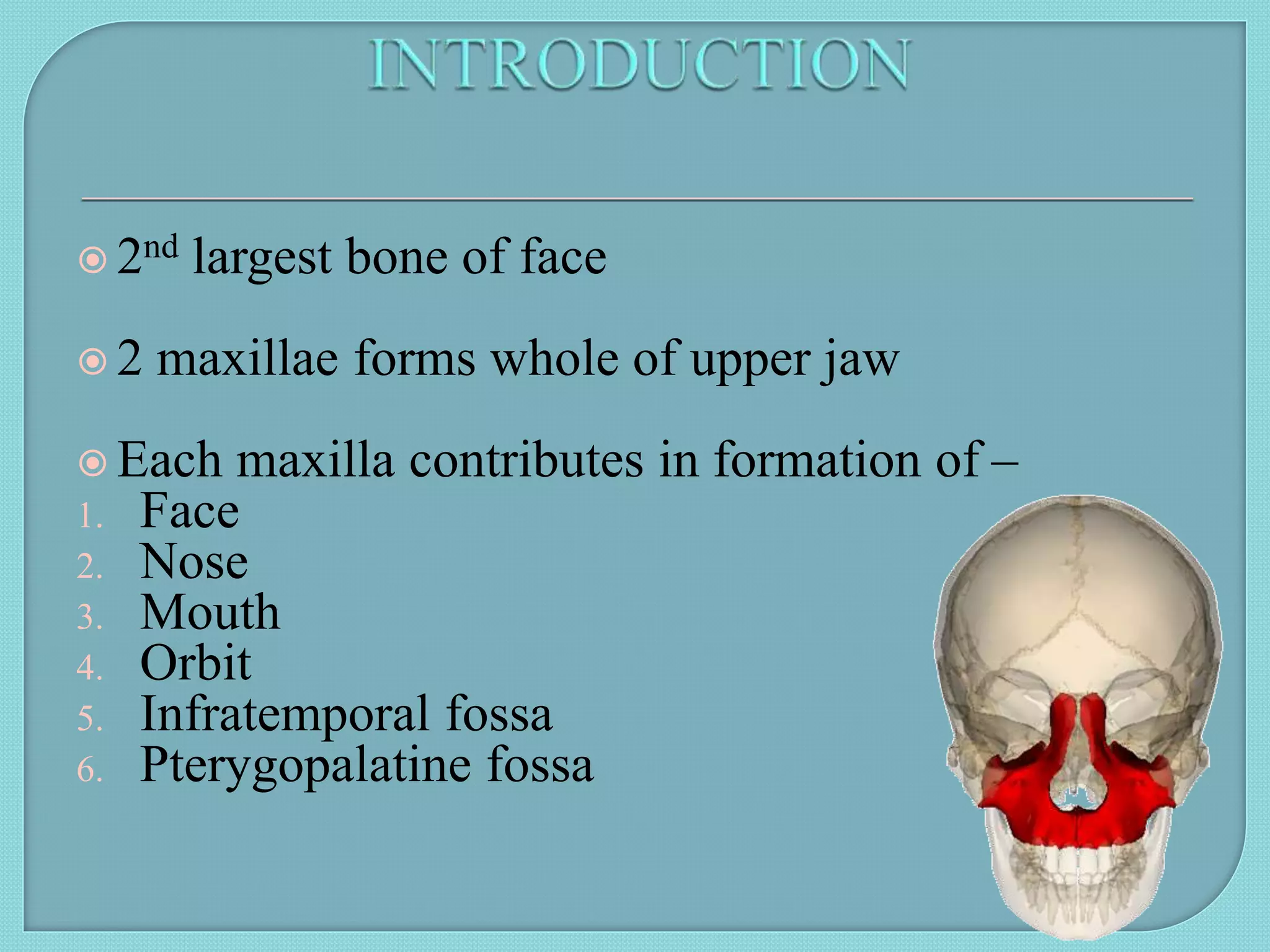
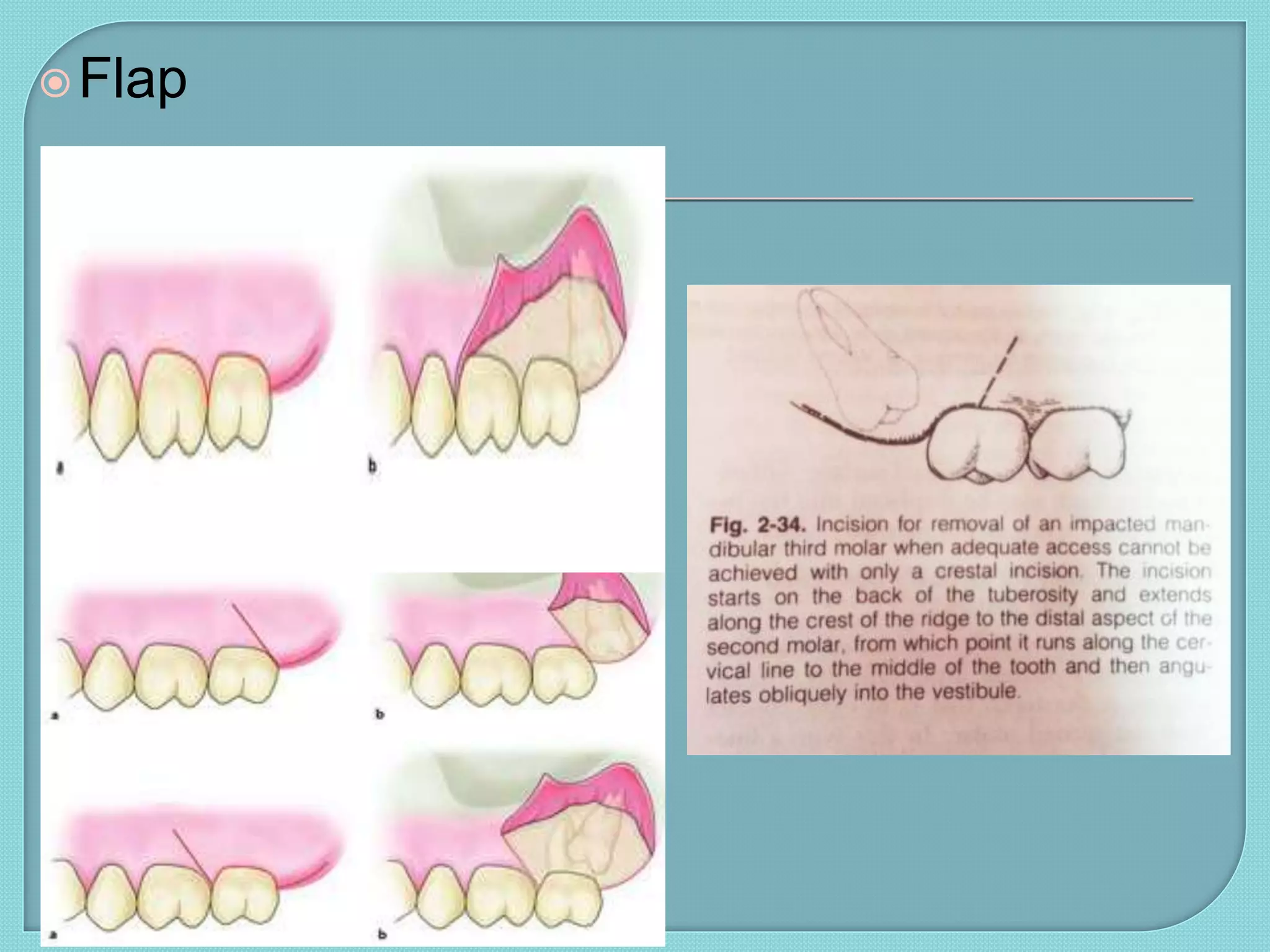
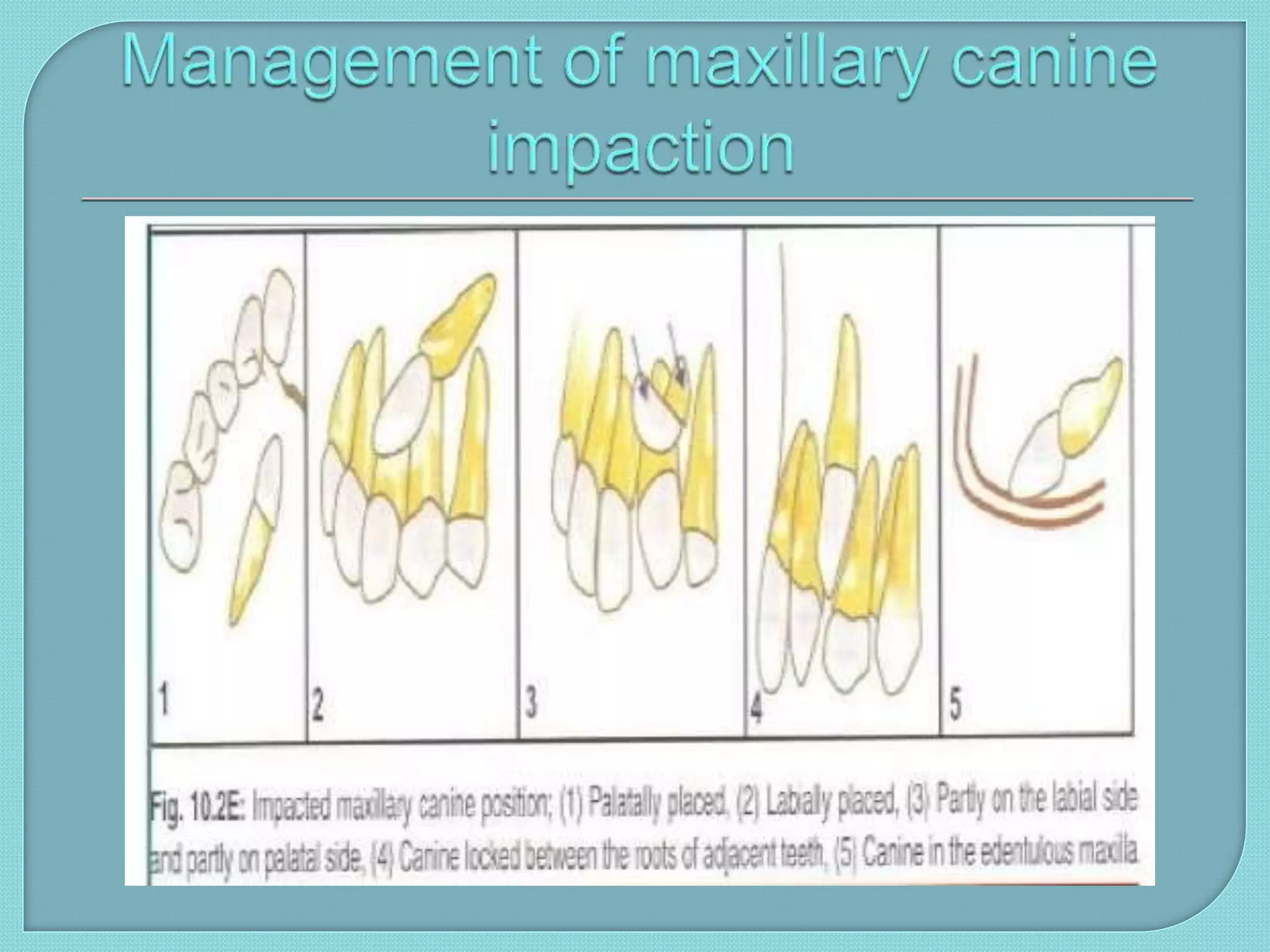
The maxilla is the second largest bone of the face that forms the upper jaw. It has a pyramidal shape with a body and four processes. It encloses the maxillary sinus and contains teeth. Unerupted and impacted teeth can occur due to various local and systemic factors. Impacted third molars and maxillary teeth are most common. Surgical removal requires careful planning including imaging and flap design. Complications may occur during surgery or postoperatively. Displaced teeth may require additional procedures like exposure through the maxillary sinus or removal from the buccal space.
![BY: KARISHMA ASHOK
[IV/I ] ROLL NO: 33](https://image.slidesharecdn.com/presentation1-160503060540/75/impacted-maxillary-3rd-molar-canine-1-2048.jpg)