Downloaded 90 times
![Q1: THE WEIRD AND WONDERFUL
What’s in the Prize Hamper? Is it:
A) Revlon cosmetics & a copy of The Hunger Games
trilogy
B) Stationery & chocolate biscuits & a cheese board
C) A single serve pack of Tic Tacs & automotive Wash
and Wax
D) A and C
E) All of the above
[1 point]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-3-320.jpg)
![Q2 : 1ST PART GLORY
Name the anatomical relations of the
oesophagus.
Posterior – possible 5 points
Anterior – possible 5 points
Left – possible 4 points
Right – possible 2 points
[16 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-4-320.jpg)
![Q3: EPONYM SCHEPONYM
Spontaneous Oesophageal Rupture, or Boerhaave
Syndrome, was first described in 1724 – True or False?
Boerhaave Syndrome was named after Dr Herman
Boerhaave, a German physician – T/F?
Boerhaave Syndrome was described in relation to Baron
Jan von Wassenaer, a Dutch Grand Admiral who sustained
a large transverse tear of his distal oesophagus due to
retching – T/F?
Baron Jan von Wassenaer had roast duck and 3 litres of
beer and a self administered emetic 3 days prior to his
death – T/F?
Herman Boerhaave had a degree in philosophy and later
became a professor of botany and medicine – T/F?
[6 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-5-320.jpg)
![Q4: TYPES AND CAUSES
Please complete the following list of types/causes of Oesophageal
Rupture:
Boerhaave’s Syndrome of “Spontaneous” Oesophageal Rupture n.b.
3 in 4 cases are preceded by vomiting
T-----
B----
P----------
I---------
E--------
P--- O-
Other
Includes caustic, peptic ulcers, foreign body, aortic pathology, diseases of
oesophagus
[6 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-6-320.jpg)
![Q5: HIGHLY MORBID
Which type of oesophageal rupture has the
highest mortality rate?
What is the main cause of death?
[2 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-7-320.jpg)
![Q6: CLINICAL PRESENTATION
Name the Mackler triad:
1
2
3
Name the Anderson triad (of clinical findings):
1
2
3
[2 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-8-320.jpg)
![Q7: CXR #1
Name the four
features of
oesophageal
rupture that are
visible on this
film.
[4 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-9-320.jpg)
![Q8: CXR #2: Name two features of oesophageal rupture
that are visible on these films. [2 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-10-320.jpg)
![Q9: CORNERSTONES OF MX
Outline the three management priorities for
oesophageal rupture
[3 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-11-320.jpg)
![Q10: TO CHOP OR NOT TO CHOP?
Name three reasons or situations that might
cause you to consider conservative (non-
operative) management of oesophageal
rupture.
[3 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-12-320.jpg)
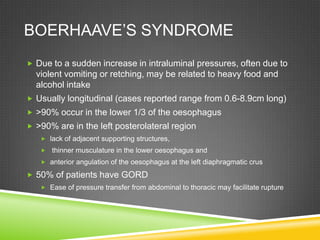
![A2 : ANATOMICAL RELATIONS OF THE
OESOPHAGUS
Name the
anatomical
relations of the
oesophagus.
Posterior –
possible 5 points
Anterior –
possible 5 points
Left – possible 4
points
Right – possible
2 points
[16 points]The lack of a serosal layer
makes it vulnerable to rupture or perforation](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-15-320.jpg)
![A3: EPONYM SCHNEPONYM
Spontaneous Oesophageal Rupture, or Boerhaave
Syndrome, was first described in 1724 – TRUE
Boerhaave Syndrome was named after Dr Herman
Boerhaave, a German physician – FALSE, he was Dutch
Boerhaave Syndrome was described in relation to Baron
Jan von Wassenaer, a Dutch Grand Admiral who sustained
a large transverse tear of his distal oesophagus due to
retching – TRUE
Baron Jan von Wassenaer had roast duck and 5 cups of
beer and a self administered emetic 3 days prior to his death
– TRUE
Herman Boerhaave had a degree in philosophy and later
became a professor of botany and medicine – TRUE
[6 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-16-320.jpg)
![A4: TYPES AND CAUSES
Please complete the following list of types/causes of Oesophageal
Rupture:
Boerhaave’s Syndrome of “Spontaneous” Oesophageal Rupture n.b.
3 in 4 cases are preceded by vomiting
Trauma
Blunt (rare – may be related to intraabdominal crush/pressure increase)
Penetrating (almost all traumas)
Iatrogenic
Endoscopy (most common cause overall)
Post Op
Other
Includes caustic, peptic ulcers, foreign body, aortic pathology, diseases of
oesophagus
[6 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-19-320.jpg)
![A5: HIGHLY MORBID
Which type of oesophageal rupture has the
highest mortality rate? – Post-emetic – ~ 30%
overall
Mortality rates reported ~2% per hour after Sx
If Rx w/in 24 hours – 25% mortality rate
If Rx after 24 hours – 65%
If Rx after 48 hours – 75-89%
No Rx – essentially 100%
What is the main cause of death? – Polymicrobial
Sepsis/Mediastinitis (+/- pleural effusion/s)
[2 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-20-320.jpg)
![Q6: CLINICAL PRESENTATION - HX
Mackler triad: (Only present in 50% of cases of Boerhaave’s)
Vomiting
Lower chest pain
Cervical subcutaneous emphysema
Typical symptoms can include:
Pain – variable location – lower anterior chest or upper abdomen most common;
may have back or neck pain. May be unable to lie flat due to pain.
Vomiting
Subcutaneous emphysema
Dysphagia or odynophagia; dysphonia
Dyspnoea
GI bleed
[1 point for naming all three ]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-21-320.jpg)
![Q6: CLINICAL PRESENTATION -
SIGNS
Name the Anderson triad (of clinical findings):
Subcutaneous emphysema
Rapid respirations
Abdominal rigidity
Physical signs may include:
Fever
Crepitus/subcutaneous emphysema
Tachycardia, shock
Tachypnoea, cyanosis, altered WOB
Upper abdominal rigidity/signs of perforation/acute abdomen
Local tenderness
Pleural effusions, pneumothorax
[1 point for naming all three ]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-22-320.jpg)
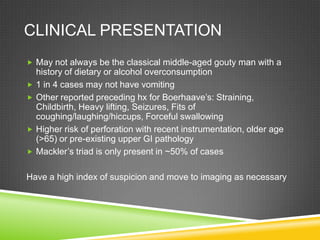
![A7: CXR
Name the four
features of
oesophageal
rupture that are
visible on this
film.
[4 points]
1. Subcut
emphysema
2. Pneumo-
mediastinum
4. Prominent renal
outline due to air
3. Air under the
diaphragm](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-24-320.jpg)
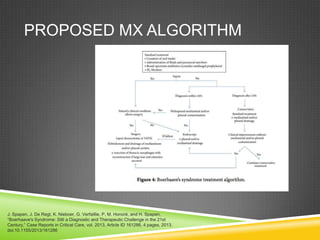
![Q8: CXR #2: Name two features of oesophageal rupture
that are visible on these films. [2 points]
1. Pneumo-
mediastinum
2. Subcut
emphysema](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-25-320.jpg)

![A9: MANAGEMENT
Aggressive resuscitation
Airway control, oxygenation, IV etc
Early surgical intervention (call Cardiothoracics!)
The time between onset of Sx and surgical intervention is the
greatest predictor of patient survival
Various thoracic procedures will depend on extent of injury:
Primary repair, stent, resection, drain placement
May need laparotomy for abdominal involvement
Broad spectrum antibiotics
To cover gram pos (incl enterococcus), gram neg and
anaerobes.
?Antifungal cover (controversial)
[3 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-27-320.jpg)
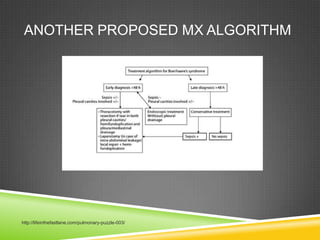
![CONSERVATIVE MANAGEMENT?
Three situations where non-operative Mx may be
considered:
Presentation >48h
Debilitated pre-morbid condition/significant comorbidity
Contained rupture with minimal symptoms and negligible
clinical evidence of sepsis (SIRS negative)
Others include
Tear not involving abdomen/contained to
mediastinum/draining to oesophagus/draining to lumen;
no neoplasm involved; no associated obstruction;
experienced thoracic surgeon available; serial contrast
imaging available
[3 points]](https://image.slidesharecdn.com/oesophagealrupture-140423220043-phpapp02/85/Oesophageal-rupture-30-320.jpg)

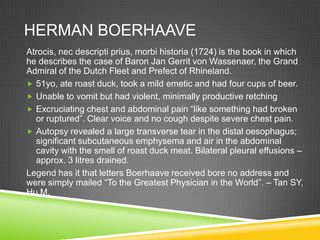
The document discusses a pub quiz on oesophageal rupture held by Dr. Deanne Chiu. It provides 10 trivia questions covering topics like the historical description of Boerhaave's syndrome, types and causes of oesophageal rupture, clinical presentation, imaging features, and management priorities. The questions test knowledge of key facts around this medical condition and its diagnosis and treatment.


































































































