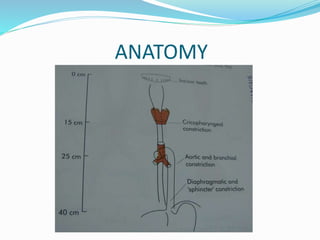
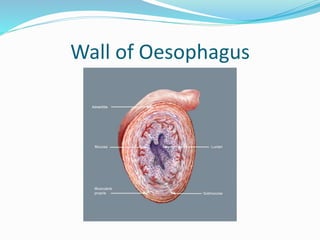
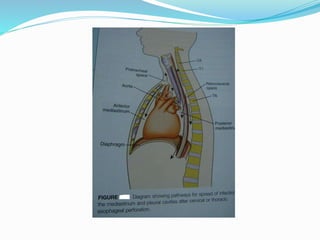
This document provides an overview of the anatomy, physiology, and common diseases of the esophagus. It begins with the learning objectives which are to understand the anatomy/physiology and clinical features of benign and malignant esophageal diseases. It then covers topics such as surgical anatomy, physiology, symptoms, investigations, congenital anomalies, foreign bodies, perforations, gastroesophageal reflux disease, hiatal hernia, motility disorders, and diverticula.















![Esophageal_Diseases_ENT_BY_NH[1].ppppptx](https://cdn.slidesharecdn.com/ss_thumbnails/esophagealdiseasesentbynh1-251115082945-26df9b86-thumbnail.jpg?width=640&height=640&fit=bounds)

























































