Downloaded 503 times


![Ophthalmic Research
Intraocular dynamic studies [fluorometry]
Tear film drainage studies
Penetration to anterior segment structures
Sharma IP](https://image.slidesharecdn.com/fluorescein-indrapsharma-150805185723-lva1-app6892/85/Fluorescein-Stain-28-320.jpg)

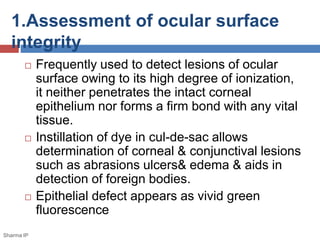
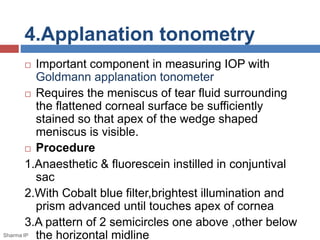
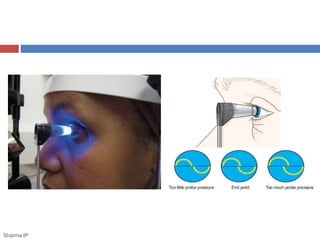
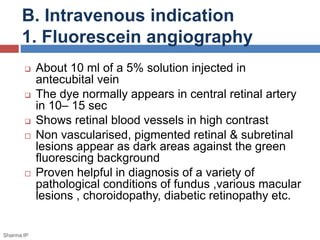
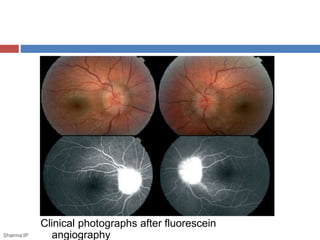
Fluorescein stain is a commonly used diagnostic agent in ophthalmology. It is a water-soluble yellow dye that appears bright green when illuminated by blue light if there is a defect or break in the corneal epithelium or conjunctiva. It has various applications including assessing ocular surface integrity, fitting contact lenses, measuring intraocular pressure, and evaluating dry eye and lacrimal drainage. While generally safe, it can cause allergic reactions through topical or intravenous use. Proper sterilization of fluorescein drops is important to prevent bacterial contamination.

















































































