- Please continue to monitor patient closely and follow up on any labs or tests ordered. Maintain NPO status, IV fluids, medications and rest as directed to support recovery from surgery. Contact medical team promptly if any concerns arise.
INTRODUCTION
Spina bifida comes from the latin word “divided spine”, is a group of neural tube
defects that involves the brain and the spinal cord and/or meninges. It occurs when the
neural tube does not close during the baby’s development. There are three major types of
spina bifida: spina bifida occulta, meningocele, and myelomeningocele. Meningocele is a
rare form of neural tube defect in which the spinal cord develops normal but the meninges
protrude from a spinal opening. Symptoms vary; while some people will have few or no
symptoms (emedTV.com). It has been reported that in 1000 live births 1-2 babies have this
kind of condition worldwide, in the Philippines it has been said that out of 86,241,691² of
the population 5,174 were reported to have spina bifida in the year 2004
(curereaserch.com).
Our patient belongs to the category of spina bifida cystica with meningocele, a mild
and rare form of neural tube defect where the spinal cord is not involved in the herniation.
He was admitted in the neuro female ward with a chief complain of headache and increase
in the head circumference. We chose this case because this is a rare condition in which it is
not commonly seen in the ward. It is an interesting case because not all have knowledge
about this condition; we want to broaden our knowledge about this case so that we may be
able to help prevent the occurrence of this condition in the community.
2.
OBJECTIVES
General Objective:
After two months of exposure at Davao Regional Hospital specifically at Ortho / Neuro
Ward, this case study aims to enhance our knowledge and understanding regarding the
diagnosis of our client so as to develop new skills in dealing with this kind of illness and to
improve our learning regarding Spina Bifida that would be helpful in our future nursing
profession.
Specific Objectives:
After this case study, we will be able to:
• Establish good interpersonal relationship with the client and his family to gain their
cooperation during the process of gathering data;
• Determine the client health status through analyzing the nature of Spina Bifida and its
deviation from the normal physiologic process;
• Trace the health history of the client and his family by taking the past and present health
history to know the predisposing and precipitating factors of client’s condition;
• Define and discuss thoroughly the complete diagnosis of the client;
• Present a through physical assessment on the client’s condition which serves as a baseline
data;
• Discuss the anatomy and physiology of the involved system in the disease;
• Trace the pathophysiology of the disease process by presenting the etiology, predisposing and
precipitating factors, its signs and symptoms present in the patient;
• Interpret the results of congregated diagnostic procedures and laboratory examinations and
its clinical significance;
• Identify and discuss the different drugs used in the management of the client’s condition;
• Formulate nursing care plan to provide adequate nursing interventions;
• Make a detailed discharge planning necessary for the wellness of the client using the acronym
METHOD;
• Interpret the general prognosis of the client base on a criteria; and
• Appreciate the experience we had upon accomplishing the said case study as well as retaining
the supplemental knowledge that we were able to acquire throughout our 2 months exposure
on the ward
3.
PERSONAL DATA
Name: PatientS
Age: 4 years old
Gender: Male
Date of Birth: November 24, 2007
Address: Southern Davao, PC, Davao Del Norte
Religion: Roman Catholic
Nationality: Filipino
Mother’s Name: Sheila
Father’s Name: Arjie
Siblings: Mayumi, Arsheil
Ordinal Position: Second among the three siblings
CLINICAL DATA
Ward: Neuro Ward
Date & Time Admitted: January 26, 2012 @ 3:30pm
Admitting Physician: Dr. Lucio Tems Jr
Chief Complain: Increasing head circumference
Addmitting Diagnosis: Spina Bifida with Non – Communicating Hydrocephalus
Final Diagnosis: Meningocoele T4 – T6 with Syringomyelia T4 – T9, Obstructive Hydrocephalus
Secondary to Chiari II Malformation
4.
HISTORY OF PATIENT
PastMedical History
During the pregnancy our patient’s mother always complies on the pre –natal check up,
she had her immunizations such as tetanus toxoid. She never took any medications that are
harmful to her pregnancy and eats foods that are good to her and to the baby. At the first
month of her pregnancy she was noted to have frequent emesis gravidarum and UTI.
Sometimes she was also expose to stress due to her work, which is a ”labandera”, and the lack
of taking supplementary vitamins.
After giving birth to our patient they noticed that there is a mass growing at the upper
back. They seek medical attention and they were advised to have a surgical intervention but
due to financial problems they refused and went home so that they could save some money for
the operation. Patient S had completed his immunizations. He has no known allergy to foods
and drugs and has only caught minor diseases such as colds, fever, and cough. At the age of 2
years old he had a convulsion; he was rushed to the hospital and was treated. But at the age of
3 years old, they noticed a slight change in patient S’s behaviour. They noticed that he has a
short temper and often cries or having a temper tantrums; they also started to notice that his
right eye and right area of his jaw cannot move, tolerable headaches and a slight increase in the
head circumference.
History of Present Illness
Three months before admission, patient S was having his check-up because of cough
and colds. As days pass, patient S was complaining of headaches, pain at the back, and they
noticed that his head is larger than any other child his age. It was then they decided to have
Shann admitted. They went to Davao Regional Hospital to seek for medical intervention and
they were advised to admit their patient for VP shunting and he was diagnosed Spina Bifida
with Non – Communicating Hydrocephalus.
Family Health Hisotry
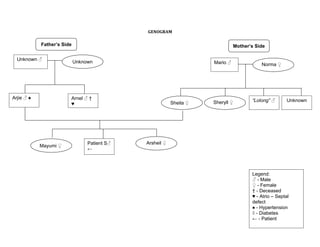
According to our source; patient S came from the Lazarito and Arguilles Clan. On the
Paternal side not much was known in the names of his Grand Father and Mother and also their
hereditary diseases. But they had two siblings namely: Arjie Arguilles and Arnel Arguilles. Arjie
was the eldest among the two and was known to have hypertension, and Arnel was the
youngest, he passed away at an early age due to a congenital condition known as the Atrio-
Septal Defect.
In the Maternal side: Mario Lazarito and Norma Lazarito where Shann’s Grand Parents;
Norma was said to have Diabetes Mellitus. They had four siblings namely: Sheila, Sheryll,
5.
“Lolong”, and theyyoungest which was not identified by our source. Shiela was the eldest
among the four and has no known hereditary condition. Sheryll on the other hand was the
second among the four and was known to have Diabetes, “Lolong” was the third and has no
known hereditary disease, and the youngest also has no known condition.
Arjie and Shiela met and got married. They were blessed with three children. Mayumi
was the eldest; she has no known hereditary condition. S, our patient, which was the second,
was known to have spina bifida, and the youngest was Arsheil who has Atrio – Septal Defect.
PHYSICAL ASSESSMENT
General Survey
Our assessment took place on February 3, 2012 at 8 am; the patient was lying flat on
bed with one pillow to elevate the head. He has a mesomorphic body built. He is slightly
kyphotic and the right shoulder is lower than the left. He was on diet as tolerated with
aspiration precaution. He has an IVF of D5.03 Nacl 500cc @ 60cc/hr, infusing well at left
metacarpal vein.
Vital Signs
Temperature: 36.8°C
Heart Rate: 108 bpm
Pulse Rate: 100 bpm
Respiratory Rate: 25 cpm
Blood Pressure: 90/60 mmHg
Skin
Our patient has a fair complexion of his skin. His skin is warm and dry to touch with
good skin turgor and with a capillary refill time of less than 3 seconds.
Head
Hair is black, shaved and evenly distributed, no infestations of lice noted upon
inspection. Head is slightly larger than normal with 52 cm in diameter. With Ventriculo –
Peritoneal Shunt at right side of the occipital area, with pinkish scar noted at the left side of the
occipital area.
Eyes
Eyes are symmetrical and are aligned at the upper pinnea of the ear. Iris is color brown
and pupils are equally round and is reactive to light accommodation with a diameter of 2 mm.
Our patient still cannot fully move the right eyelids, though can fully move the eyeballs from
side-to-side and up and down. Sunken eyeballs noted upon inspection.
Ears
Ears are symmetrical and are aligned at the outer canthus of the eye. Eardrums are
intact with cerumen noted upon inspection. No lesions, discharges noted.
Nose
Nose is symmetrically aligned at the center of the head. No discharges noted upon
inspection
Neck and Throat
Patient was able to swallow. Upon palpation there was no mass noted.
8.
Mouth
Lips and the oral mucosa are pinkish in color with no lesion noted. The right side of the
jaw is slightly slanted.
Chest
Chest is normal in shape, with AP diameter of 2:1. Right shoulder is lower than the left
shoulder. At the upper back, suture lines noted.
Abdomen
The abdomen is flat and is light brown in color with a bowel sound of 5. No lesions
noted upon inspection.
Genio – Urinary
At his age, patient is able to hold his bladder for a long time.
Upper Extremities
Upper extremities are symmetrical in shape and size, and able to move both extremities
without difficulty. No lesions noted upon inspection.
Lower Extremities
Lower extremities are symmetrical in shape and size, with small scars noted at the shin
part of the leg.
9.
COURSE IN THEWARD
Date and Time Doctor’s Order Nurse’s Care
1/26/12 -Please admit patient under -VS checked and recorded
3: 30 pm neurosurgery ward -Secured consent to care
Temp. 36 -Secure consent to care - DAT / NPO post midnight re-
BP: 90/60 -I & O q shift instructed
PR: 129 bpm -vs q 4 -I & O q shift recorded
RR: 24 - DAT / NPO post midnight -Followed up lab exams
- For VP shunting once with pedia requested
clearance
- Senior informed
- Meds:
Ranitidine 15mg IVTT q8 once on
NPO
IVF D5.3 Nacl 500cc @ 50-55 cc/hr
- Laboratory examinations:
CBC with BT, PT / APTT, Na, K, Ca,
Creatinine, CXR APL
1/27/12 -Followed – up all labs -Labs followed up
7:00 am -Followed – up official reading of CXR -Informed Radiologic Dept.
- For pedia clearance once with Official reading CXR
complete lab work – up - May have DAT
-DAT
1/28/12 -Will do ECG 12 leads with long lead -ECG 12 leads taken
8:15 am II -D/C Ranitidine as ordered
-D/C Ranitidine
1/29/12 -D/C IVF once comsumed -IVF consumed and
8:00 am -Refer to Pedia tomorrow once with terminated
complete labs -For referral to Pedia once
with with complete labs,
followed up labs
1/30/12 -Follwed up Official Reading of CXR -Informed Official reading
7:00 am CXR, to retrieve X ray film
7:00 pm -For cranial CT Scan ( Plain ) -Instructed S.O for cranial CT
Scan
1/31/12 -Refer to Pediatrics for CP clearance -Informed Pediatrics for CP
10.
9:00 am Clearance
5:15 pm -Secure 1 unit of PRBC of Pt’s blood -Informed S.O. to secure
type properly screened & blood for OR use, blood
crossmatched for OR use request and crossmatching
given
2/1/12 -NPO post midnight -Instructed watcher that
9:51 am -Schedule for VP shunting, Repair of patient should be on NPO
Meningocele tomorrow 1st table starting midnight
- Secure consent and procdure - Secured consent of the
-Inform OR/Anesthesia procedure
-Start Cefuroxime 350mg IVTT ANST - Scheduled elective VP
1 hr prior shunting and repair of
meningocele tomorrow
- OR/AROD aware
- Skin testing done with result
of negative; cefuroxime
started IVTTT
2:40 pm - Provided with CP clearance. Pls -Informed Dr. Daya and Dr.
informed Dr. Daya / Dr. Bravo Bravo
3 pm Pre op orders -Followed up availability of
- For elective VP shunt and repair of meds
meningocele under GETA
- NPO
-Meds:
1. Ranitidine 15mg IVTT PTOR
2. Metoclopromide 5mg IVTT PTOR
5:45 pm - Insert IV D5.3NaCl 500cc x 60cc/hr - IVF started D5.3NaCl 500cc
@ 60cc/hr at midnight
- Instructed to wear gown
- Removed any metallic
objects
- Pre op meds given IVTT prior
to OR
11.
2/2/12 Post Op orders: -Maintain NPO as ordered
4:00 pm -S/P VP shunting & Repair of -Hooked to O2 inhalation via
Meningocele under GETA face mask @ 6 liters per
-To PACU minute
-NPO Temporarily -VS checked and monitored
-O2 @ 6 liter per minute via face -IVF D5.3 Nacl 400cc @ 60cc/
mask hr, regulated well
-VS q15 minutes x 3 takings then q15 -Due meds given as ordered
minutes -I & O monitored
-Maintain flat on bed for 24 hours
-IVF D5.3 Nacl 400 @ 60 cc/hr
-Meds:
Cefuroxime 300 mg IVTT q8h
Ranitidine 20 mg IVTT q8h
Tramadol 30 mg IVTT q8h
Paracetamol 300 mg IVTT q6h RTC
for pain
-Monitor I & O q hourly
- Repeat CBC post op
-Keep pt. warm
-Refer
7 pm - To ward - Transferred out to ward per
- NPO temporarily stretcher, endorsed to NOD
- continue IVTT meds - Still on NPO
- please follow up laboratory request - Due meds given
2/3/12 -May have DAT with SAP - Resumed Diet as tolerated
-Still flat on bed -instructed to maintain flat on
-IVF D5.3 Nacl @ 60 cc/hr bed
-Continue all meds -IVF regulated @ prescribed
rate
-Due meds available given as
ordered
2/4/12 -May elevate head with 1 pillow -Elevated head with 1 pillow
6:00 am -refer
2/5/12 -For dressing tomorrow - Dressing c/o ROD, followed
8:00 am -Continue IVF up availability of materials
-IVF regulated well at
prescribed rate
12.
2/6/12
8:00 am -Decrease IVF to 50 cc/hr -IVF decreased to 50 cc/hr,
-D/C Tramadol & Ranitidine regulated well
- Change dressing -D/C Tramadol & Ranitidine
IVTT
2/7/12 -May now remove IVF - IVF consumed and
6:50 pm -Shift IV Meds to P.O discontinued
Cefixime 100mg/5ml, 7ml BID -Shifted to PO meds
Paracetamol 250mg/5ml, 5ml q4 - PO meds started
PRN for fever
2/8/12 -May Go Home -Carried out MGH ordered
10:00 am -Home Meds as ordered x 7 days -Discharged plan made
Cefixime 100mg/5ml, 7ml BID - Bills forwarded
Paracetamol 250mg/5ml, 5ml q4 -Instructed take home meds
PRN for fever -health teachings imparted
-Neuro Surgery OPD check up on -Discharged ambulatory
Feb.16, 2012 8-10 am
13.
Anatomy and Physiology
Brain- The brain is the center of the nervous system. The function of the brain is to provide
coherent control over the actions of an animal. A centralized brain allows groups of muscles to
be co-activated in complex patterns; it also allows stimuli impinging on one part of the body to
evoke responses in other parts, and it can prevent different parts of the body from acting at
cross-purposes to each other. To generate purposeful and unified action, the brain first brings
information from sense organs together at a central location. It then processes this raw data to
extract information about the structure of the environment. Next it combines the processed
sensory information with information about the current needs of an animal and with memory
of past circumstances. Finally, on the basis of the results, it generates motor response patterns
that are suited to maximize the welfare of the animal. These signal-processing tasks require
intricate interplay between a variety of functional subsystems
The brain is one of the largest and most complex organs in the human body.
It is made up of more than 100 billion nerves that communicate in trillions of connections called
synapses.
The brain is made up of many specialized areas that work together:
• The cortex is the outermost layer of brain cells. Thinking and voluntary movements begin in
the cortex.
• The brain stem is between the spinal cord and the rest of the brain. Basic functions like
breathing and sleep are controlled here.
• The basal ganglia are a cluster of structures in the center of the brain. The basal ganglia
coordinate messages between multiple other brain areas.
• The cerebellum is at the base and the back of the brain. The cerebellum is responsible for
coordination and balance.
The brain is also divided into several lobes:
• The frontal lobes are responsible for problem solving and judgment and motor function.
• The parietal lobes manage sensation, handwriting, and body position.
• The temporal lobes are involved with memory and hearing.
• The occipital lobes contain the brain's visual processing system.
The brain is surrounded by a layer of tissue called the meninges. The skull (cranium) helps
protect the brain from injury.
Brain stem - The brain stem is similarly structured as the spinal cord: it consists of grey matter
surrounded by white matter fibre tracts. Its major regions are the midbrain, pons and medulla
oblongata. The midbrain, which surrounds the cerebral aqueduct, provides fibre pathways
between higher and lower brain centres, contains visual and auditory reflex and subcortical
motor centres. The pons is mainly a conduction region, but its nuclei also contribute to the
regulation of respiration and cranial nerves. The medulla oblongata takes an important role as
an autonomic reflex centre involved in maintaining body homeostasis. In particular, nuclei in
the medulla regulate respiratory rhythm, heart rate, blood pressure and several cranial nerves.
14.
Moreover, it providesconduction pathways between the inferior spinal cord and higher brain
centres.
Cerebellum - The cerebellum, which is located dorsal to the pons and medulla, accounts for
about 11% of total brain mass. Like the cerebrum, it has a thin outer cortex of grey matter,
internal white matter, and small, deeply situated, paired masses (nuclei) of grey matter. The
cerebellum processes impulses received from the cerebral motor cortex, various brain stem
nuclei and sensory receptors in order to appropriately control skeletal muscle contraction, thus
giving smooth, coordinated movements.
Cerebral hemispheres - The cerebral hemispheres, located on the most superior part of the
brain, are separated by the longitudinal fissure. They make up approximately 83% of total brain
mass, and are collectively referred to as the cerebrum. The cerebral cortex constitutes a 2-4
mm thick grey matter surface layer and, because of its many convolutions, accounts for about
40% of total brain mass. It is responsible for conscious behaviour and contains three different
functional areas: the motor areas, sensory areas and association areas. Located internally are
the white matter, responsible for communication between cerebral areas and between the
cerebral cortex and lower regions of the CNS, as well as the basal nuclei (or basal ganglia),
involved in controlling muscular movement.
Cerebrospinal fluid - Cerebrospinal fluid (CSF) is a watery liquid similar in composition to blood
plasma. It is formed in the choroid plexuses and circulates through the ventricles into the
subarachnoid
space, where it is returned to the dural venous sinuses by the arachnoid villi. The prime
purpose of the CSF is to support and cushion the brain and help nourish it.
CSF serves four primary purposes:
1.Buoyancy: The actual mass of the human brain is about 1400 grams; however, the net weight
of the brain suspended in the CSF is equivalent to a mass of 25 grams. The brain therefore
exists in neutral buoyancy, which allows the brain to maintain its density without being
impaired by its own weight, which would cut off blood supply and kill neurons in the lower
sections without CSF.
2.Protection: CSF protects the brain tissue from injury when jolted or hit. In certain situations
such as auto accidents or sports injuries, the CSF cannot protect the brain from forced contact
with the skull case, causing hemorrhaging, brain damage, and sometimes death.
3.Chemical stability: CSF flows throughout the inner ventricular system in the brain and is
absorbed back into the bloodstream, rinsing the metabolic waste from the central nervous
system through the blood-brain barrier. This allows for homeostatic regulation of the
distribution ofneuroendocrine factors, to which slight changes can cause problems or damage
to the nervous system. For example, high glycine concentration disrupts temperature and blood
pressure control, and high CSF pH causes dizziness and syncope.
4.Prevention of brain ischemia: The prevention of brain ischemia is made by decreasing the
amount of CSF in the limited space inside the skull. This decreases total intracranial pressure
and facilitates blood perfusion.
15.
Dermatomes and Myotome- Each spinal nerve pair services specific areas of the body with
sensory and motor neurons. The sensory nerve fibers and the areas of the skin they receive
stimulus from are called dermatomes. The motor nerve fibers and the specific muscles which
they effect are called myotomes.
Diencephalon - The diencephalon is located centrally within the forebrain. It consists of the
thalamus,
hypothalamus and epithalamus, which together enclose the third ventricle. The thalamus acts
as a grouping and relay station for sensory inputs ascending to the sensory cortex and
association areas. It also mediates motor activities, cortical arousal and memories. The
hypothalamus, by controlling the autonomic (involuntary) nervous system, is responsible for
maintaining the body’s homeostatic balance. Moreover it forms a part of the limbic system, the
‘emotional’ brain. The epithalamus consists of the pineal gland and the CSF producing choroid
plexus.
Meninges - The meninges are three connective tissue membranes enclosing the brain and the
spinal cord. Their functions are to protect the CNS and blood vessels, enclose the venous
sinuses, retain the cerebrospinal fluid, and form partitions within the skull. The outermost
meninx is the dura mater, which encloses the arachnoid mater and the innermost pia mater.
Spinal Cord - The spinal cord is a long, thin, tubular bundle of nervous tissue and support cells
that extends from the brain (the medulla oblongata specifically). The spinal cord begins at the
occipital bone and extends down to the space between the first and second lumbar vertebrae;
it does not extend the entire length of the vertebral column. It is around 45 cm (18 in) in men
and around 43 cm (17 in) long in women. Also, the spinal cord has a varying width, ranging from
1/2 inch thick in the cervical and lumbar regions to 1/4 inch thick in the thoracic area. The
enclosing bony vertebral column protects the relatively shorter spinal cord. The spinal cord
functions primarily in the transmission of neural signals between the brain and the rest of the
body but also contains neural circuits that can independently control numerous reflexes and
central pattern generators. The spinal cord has three major functions: as a conduit for motor
information, which travels down the spinal cord, as a conduit for sensory information in the
reverse direction, and finally as a center for coordinating certain reflexes.
16.
ETIOLOGY
PREDISPOSING FACTORS
Rationale
Age ♦ Infants and children are more likely to have
this condition because it is a birth defect.
Heredity Couples who have spina bifida are more
likely to have a child with spina bifida.
Individuals who have had spina bifida are at
risk of having a child with the same
condition.
Unknown Until now the cause of spina bifida is still
unknown. Experts still some theory as to
what is the cause of this condition.
PRECIPITATING FACTORS
Rationale
Nutrition ♦ women who do not take folic acid or lack of
folic acid prior to pregnancy and/or during
early pregnancy have a higher risk of having
spina bifida than women who take folic acid.
Anti convulsants Valproic acid and carbamazepine belong to a
group of drugs called folic acid antagonist.
This group interferes with the body’s use of
folic acid.
Socio-economic factors ♦ Socio-economic status of the person would
also affect the risk of having spina bifida
because of the decrease compliance of
nutrition and supplements of the mother
during pregnancy.
Diabetes Women who have diabetes before they
become pregnant are at higher risk of having
a child with spina bifida and other types of
birth defects.
Increase body temperature Studies suggest that if a woman’s body
temperature goes up to 101 - 102°F (38.33 –
38.88°C) during early pregnancy, it would
double the risk of having a child with spina
bifida.
17.
PATHOPHYSIOLOGY
During the first month of pregnancy the upper part of the spinal cord and the brain is
formed, followed by the formation of the lower spinal cord at 5 – 6 weeks during pregnancy. An
interruption in the formation would result to failure in closure of the spinal cord leaving a
defect in the spine. Factors affecting failure of closure would include the inadequate folic acid
intake which is used by the body for cell production and development; anticonvulsant which is
a folic acid antagonist blocks the absorption of folic acid. Having a history of diabetes before or
during pregnancy with high levels of glucose in the body would also affect the closure of the
spine as well as having a high body temperature during pregnancy.
In the first month of pregnancy, the central nervous system of the baby starts to
develop. Any slight interruption of the development will lead to a congenital defect. If it will
occur, there will be a defect in the spinal cord in which the neural tube will fails to close thus
creating an opening and forms a protrusion of the meninges through the spinal space and what
is now called the “Meningocele”. If treated through surgical repair of meningocele it would lead
to a good prognosis. But if not, the protrusion will create an obstruction. Due to the
obstruction, there will be an indirect flow of cerebro-spinal fluid in and out of the spinal cord
and it will accumulate in the brain creating now a hydrocephalus. Hydrocephalus if treated with
VP shunt would either lead to a good prognosis or would create a shunt complication including
shunt malfunction, clogged VP shunt or infection. If not treated, the CSF will still continue to
accumulate in the brain and in the long term the person would develop learning disabilities and
would further complicate to mental retardation. Meanwhile if there is a continuous
accumulation of the CSF, it cannot circulate properly and would force its way below the spinal
cord. If that happens there would be a displacement of the foramen magnum and creates a
herniation of the cerebellum, this condition is called Chiari II malformation in which the person
would experience headache, nausea and vomiting, dizziness, increased intra cranial pressure. If
not treated there would be a compression of the spinal cord making the person feel choking
sensation, arm stiffness, difficulty in feeding, swallowing and breathing and eventually would
die.
18.
Predisposing factors: Precipitating factors:
- Age - Nutrition
- Heredity - Medications
- Unknown - Socio-economic factors
-Diabetes
- Increased body temp
1st month of
Central Nervous
System begins to
form
Defect in the spinal
Defect in the closure
of the neural tube
Protruding sac
through the defect-
containing meninges
Dx:
- Meningocele
Translumination
- CT scan
- MRI
If treated: If not
- Surgical repair of No direct flow of CSF to
menigocele the spinal cord
Good
Obstruction of
prognosis
fluid in the
brain
CSF unable to
circulate
19.
Accumulation of CSF
s/sx: Hydrocephal
in the brain
- increased us
ICP
- increase Fluid may
head possibly forced
circumferenc
Displacement of
foramen
If treated: If not magnum
treated:
Chiari II
- VP Fluid still malformation
accumulated in the
s/sx:
Good Shunt - headache - muscle
prognosis complication Learning weakness
disabilities - nausea - increased ICP
- dizziness
s/sx:
Mental
- headache
retardation If not treated:
- nausea &
vomiting
- fever Compression
of the spinal
cord
s/sx:
- choking,
- arm stiffness
- difficulty in feeding,
swallowing, and
20.
IDEAL SURGICAL MANAGEMENTOF THE CONDITION
Diagnostic Exams in Detecting Spina Bifida
During Pregnancy:
1. Amniocentesis – a test that involves taking a sample of the mother’s amniotic fluid through a
needle inserted into a womb of a mother. Elevated levels of AFP, a gamma 1
globulin, indicates the presence of neural tube defects.
2. Ultrasound
After Pregnancy:
1. Translumination – a test where a light a shined through the sac to determine the structure of
the sac. If the light is translucent it is meningocele, if not translucent would
indicate that it is meningomyelocele.
2. CT Scan
3. MRI
Surgical Intervention of Spina Bifida:
1. Repair of meningocele
2. AV shunt
21.
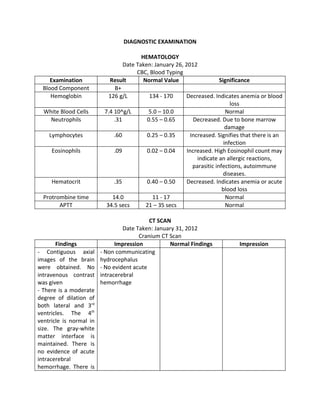
DIAGNOSTIC EXAMINATION
HEMATOLOGY
Date Taken: January 26, 2012
CBC, Blood Typing
Examination Result Normal Value Significance
Blood Component B+
Hemoglobin 126 g/L 134 - 170 Decreased. Indicates anemia or blood
loss
White Blood Cells 7.4 10^g/L 5.0 – 10.0 Normal
Neutrophils .31 0.55 – 0.65 Decreased. Due to bone marrow
damage
Lymphocytes .60 0.25 – 0.35 Increased. Signifies that there is an
infection
Eosinophils .09 0.02 – 0.04 Increased. High Eosinophil count may
indicate an allergic reactions,
parasitic infections, autoimmune
diseases.
Hematocrit .35 0.40 – 0.50 Decreased. Indicates anemia or acute
blood loss
Protrombine time 14.0 11 - 17 Normal
APTT 34.5 secs 21 – 35 secs Normal
CT SCAN
Date Taken: January 31, 2012
Cranium CT Scan
Findings Impression Normal Findings Impression
- Contiguous axial - Non communicating
images of the brain hydrocephalus
were obtained. No - No evident acute
intravenous contrast intracerebral
was given hemorrhage
- There is a moderate
degree of dilation of
both lateral and 3rd
ventricles. The 4th
ventricle is normal in
size. The gray-white
matter interface is
maintained. There is
no evidence of acute
intracerebral
hemorrhage. There is
22.
no midline shift
-The cortical sulci
cisterns, sella and CP
angles are normal for
patients stated age.
- The visualized
paranasal sinuses and
mastoid air cells are
pneumatised.
- The visualized
cranium is intact.
HEMATOLOGY
Date Taken: February 2, 2012
CBC
EXAMINATION RESULT NORMAL SIGNIFICANCE
VALUE
Hemoglobin 103 g/L 134 - 170 Decreased when there is anemia, or blood
loss due to surgery, or active bleeding
WBC 13.6 ^g/L 5.0 – 10.0 Increased. May be increased with infection
or inflammation.
Neutrophils 0.69 0.55 – 0.65 Increased. May be due to infection,
inflammation or stress
Lymphocytes 0.27 0.25 – 0.35 Normal
Hematocrit 0.29 0.40 – 0.50 Decreased, when there is anemia or blood
loss due to surgery.
CLINICAL CHEMISTRY
Date Taken: February 2, 2012
FBS
EXAMINATION RESULT NORMAL VALUE SIGNIFICANCE
Fasting Blood Sugar 3.48 mmol/L Adults: 4.11- 5.58 mmol/L Normal
60 -90 yrs.: 4.56 – 6.38
mmol
> 90 yrs.: 4.16- 6.72 mmol/L
Children: 3.33 – 5.55 mmol/
L
23.
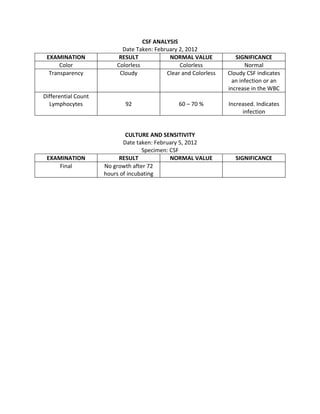
CSF ANALYSIS
Date Taken: February 2, 2012
EXAMINATION RESULT NORMAL VALUE SIGNIFICANCE
Color Colorless Colorless Normal
Transparency Cloudy Clear and Colorless Cloudy CSF indicates
an infection or an
increase in the WBC
Differential Count
Lymphocytes 92 60 – 70 % Increased. Indicates
infection
CULTURE AND SENSITIVITY
Date taken: February 5, 2012
Specimen: CSF
EXAMINATION RESULT NORMAL VALUE SIGNIFICANCE
Final No growth after 72
hours of incubating
24.
DRUG STUDY
RANITIDINE
Generic Name: Ranitidine hydrochloride
Brand Name: Zantac
Classification: H2 Histamine Receptor Antagonist
Ordered Dose: 1/26/12 15mg IVTT q 8hrs once on NPO
2/1/12 15mg IVTT prior to OR
2/2/12 20mg IVTT q 8hrs
Mode of Action: Competitively inhibits action of H2 at receptor sites of parietal cells,
decreasing gastric acid secretion which relieves GI discomfort
Indication:
Pre operative: to relieve GI discomfort from NPO patients
Post operative: to counter the effects of NSAIDS, this causes an increase in gastric
secretions
Contraindications:
• Use cautiously in elderly patients.
• Use cautiously in patients with hepatic dysfunction.
Drug Interaction:
• Antacids may interfere with ranitidine absorption
• Deceases diazepam absorption
• Smoking may increase gastric acid secretion and worsen disease
• It may interfere with warfarin clearance, monitor patient closely for bleeding
Side Effects:
CNS: headache, dizziness
Ophtha: blurred vision
GI: constipation, nausea, vomiting, diarrhea, hepatotoxicity
GU: gynecomastia
Systemic: Anaphylaxis, Angioedema
Nursing Responsibilities:
1. Observe the 5 basic rights of drug administration before giving the drug.
2. Explain the purpose of the drug given to the patient.
3. Explain to the patient for any side effects of the drug.
3. Instruct the patient not to have activities which requires high alertness such as running,
walking.
4. Encourage the patient to eat high fiber foods and increase oral fluid intake because
constipation might occur as side effect.
5. Instruct the patient to report any signs of hepatotoxicity such as: dark colored urine,
clay-colored stool, yellow skin or sclera, itching.
25.
Mectoclopromide
Generic Name: Metoclopramidehydrochloride
Brand Name: Apo-Metoclop
Classification: Antiemetic
Ordered Dose: 2/1/12 5mg IVTT prior to OR
Mode of Action: Stimulates motility of upper GI tract by increasing lower esophageal
sphincter tone. Blocks chemoreceptor trigger zone which prevents or
minimizes nausea and vomiting. Also reduces gag reflex, improves gastric
emptying and reduces gastric reflux.
Indication: To prevent or reduce postoperative nausea and vomiting.
Contraindication:
• Use cautiously in patients with a history of depression, Parkinson’s disease,
hypertension or renal impairment. Also contraindicated in patients taking drugs
that are likely to cause extrapyramidal reactions and those with seizure disorders.
Drug Interaction:
• Alcohol use may cause additive CNS depression. Discourage using together.
• Anticholinergics may antagonize GI motility effects of metoclopramide.
• Acetaminophen, aspirin, cyclosporine, diazepam, and levodopa may increase the
absorption of these drugs. Watch closely for adverse effects.
Adverse Reaction:
CNS: sedation, fatigue, headache
GI: dry mouth, constipation, nausea and vomiting, diarrhea
GU: decrease libido
CV: hypotension, bradycardia
Systemic: rashes
Nursing responsibilities:
1. Observe the 5 basic rights in drug administration before giving the drug to the patient.
2. Explain the purpose of the drug to the patient.
3. Explain for any side effects that might occur after giving the drug.
4. Instruct the patient or significant other that sedation might occur as side effect and be
careful when doing something to prevent further injuries.
5. Instruct patient to increase oral fluid intake.
6. Instruct the patient or significant other not to rise on bed immediately to prevent
orthostatic hypotension.
7. Encourage patient to eat foods rich in fiber.
26.
CEFIXIME
Generic Name: Cefixime
BrandName: Suprax
Classification: Third- Generation Cephalosporin; Antibiotic
Ordered Dose: 2/7/12 100mg/5ml 7ml BID PO
Mode of Action: Inhibits cell wall synthesis, preventing osmotic instability; usually
bactericidal which hinders or kills bacteria, including H. influenza, M.
catarrhalis, S. pyogenes, S. pneumonia, E. coli, and P. mirabilis.
Indication: To prevent infection especially for post operative patients
Contraindication:
• Contraindicated in patients hypersensitive to drug, other cephalosporins and
penicillins.
Drug Interaction:
• Aluminum antacids and magnesium may reduce cefditoren absorption. Avoid using
together. If used together, separate doses.
Adverse Reaction:
CNS: headache, dizziness
GI: nausea and vomiting, diarrhea, abdominal pain
GU: nephrotoxicity
Integ: rash, urticaria
Respi: dyspnea
Systemic: anaphylaxis
Nursing responsibilities:
1. Observe the 5 basic rights of drug administration before giving the drug to the patient.
2. Check for any allergies of the drug.
3. Explain the purpose of the drug to the patient.
4. Explain for any side effects that might occur after giving the drug.
5. Advice patient to have light to moderate meal before giving this drug.
6. Instruct patient to report signs of allergic reactions to the drug such as: rashes, urticaria,
dyspnea,
7. Instruct patient to report for signs of nephrotoxicity.
CEFUROXIME
27.
Generic Name: Cefuroximesodium
Brand Name: Zinacef
Classification: Second - Generation Cephalosphorin; Antibiotic
Ordered Dose: 2/2/12 300mg IVTT q 8hrs ANST
Mode of Action: Inhibits cell-wall synthesis, promoting osmotic instability; usually
bactericidal which hinders or kills susceptible bacteria, including many
gram-positive organisms and enteric gram-negative bacilli.
Indication: Post - operative prophylaxis for infection
Contraindication:
• Contraindicated in patients hypersensitive to drug and other drug cephalosporins.
Drug interaction:
• Diuretics may increase risk of adverse renal function
• Probenicid may inhibit excretion and increase level of cefuroxime. Sometimes used
for this effect.
• Any food may increase drug absorption and bioavailability of suspension. Give
suspension with food. Tablets may be given without regard to food.
Adverse Reaction:
CNS: dizziness, headache
GI: diarrhea, nausea and vomiting, abdominal cramps
GU: nephrotoxicity
Systemic: anaphylaxis
Nursing responsibilities:
1. Observe the 5 basic rights of drug administraiton before giving the drug to the patient.
2. Check for any allergies of this drug by doing skin testing.
3. Explain the purpose of the drug to the patient.
4. Explain possible side effects that might occur after giving the drug.
5. Advice the patient to have light to moderate meal before giving the drug.
6. Instruct the patient for signs of allergic reaction such as: rashes, urticaria, dyspnea,
edema, itching, swelling
PARACETAMOL
28.
Generic Name: Acetaminophen
BrandName: Paracetamol, Tylenol
Classification: Antipyretic, Analgesic, Anti inflammatory
Ordered dose: 2/2/12 300mg IVTT q 6hrs RTC for pain
2/7/12 250mg/5ml 5ml q 4hrs PRN for fever
Mode of Action: Block pain impulses peripherally that occur in response to inhibition of
prostaglandin synthesis; anti pyretic action results from inhibition of
prostaglandin in the CNS
Indication: to relieve mild pain, to relieve or prevent fever
Contraindication: contraindicated to patients hypersensitive to the drug, patients with
problems in the liver
Side Effects:
CNS: drowsiness
GI: nausea and vomiting, diarrhea, hepatotoxicity
Integ: rash, urticaria
Nursing Responsibilities:
1. Observe the 5 basic rights in drug administration before giving the drug to the patient.
2. Explain the purpose of giving the drug.
3. Explain to the patient the possible side effects of the drug.
4. Instruct the patient not to overdose as it is harmful to the liver.
5. Instruct patient to report signs of hepatotoxicity such as: dark colored urine, jaundice,
icteric sclera, itching.
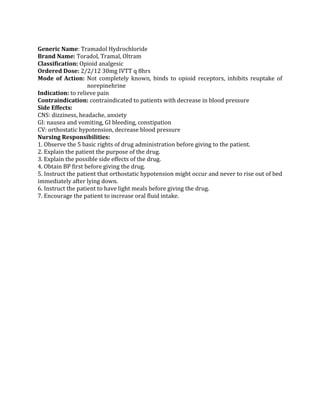
TRAMADOL
29.
Generic Name: TramadolHydrochloride
Brand Name: Toradol, Tramal, Oltram
Classification: Opioid analgesic
Ordered Dose: 2/2/12 30mg IVTT q 8hrs
Mode of Action: Not completely known, binds to opioid receptors, inhibits reuptake of
norepinehrine
Indication: to relieve pain
Contraindication: contraindicated to patients with decrease in blood pressure
Side Effects:
CNS: dizziness, headache, anxiety
GI: nausea and vomiting, GI bleeding, constipation
CV: orthostatic hypotension, decrease blood pressure
Nursing Responsibilities:
1. Observe the 5 basic rights of drug administration before giving to the patient.
2. Explain the patient the purpose of the drug.
3. Explain the possible side effects of the drug.
4. Obtain BP first before giving the drug.
5. Instruct the patient that orthostatic hypotension might occur and never to rise out of bed
immediately after lying down.
6. Instruct the patient to have light meals before giving the drug.
7. Encourage the patient to increase oral fluid intake.
30.
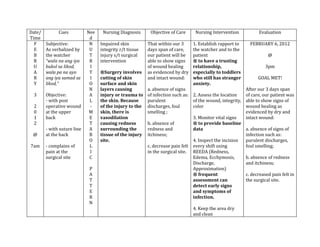
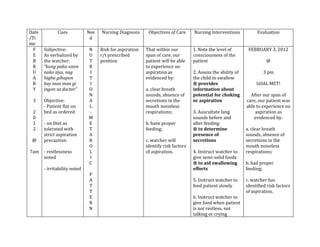
Date/ Cues Nee Nursing Diagnosis Objective of Care Nursing Intervention Evaluation
Time d
F Subjective: N Impaired skin That within our 3 1. Establish rapport to FEBRUARY 6, 2012
E As verbalized by U integrity r/t tissue days span of care, the watcher and to the
B the watcher T injury s/t surgical our patient will be patient @
R “wala na ang iya R intervention able to show signs ® to have a trusting
U bukol sa likod, I of wound healing relationship, 3pm
A wala pa na ayo T ®Surgery involves as evidenced by dry especially to toddlers
R ang iya samad sa I cutting of skin and intact wound: who still has stranger GOAL MET!
Y likod,” O surface and skin anxiety.
N layers causing a. absence of signs After our 3 days span
3 Objective: A injury or trauma to of infection such as: 2. Assess the location of care, our patient was
- with post L the skin. Because purulent of the wound, integrity, able to show signs of
2 operative wound - of the injury to the discharges, foul color wound healing as
0 at the upper M skin, there is smelling ; evidenced by dry and
1 back E vasodilation 3. Monitor vital signs intact wound:
2 T causing redness b. absence of ® to provide baseline
- with suture line A surrounding the redness and data a. absence of signs of
@ at the back B tissue of the injury itchiness; infection such as:
O site. 4. Inspect the incision purulent discharges,
7am - complains of L c. decrease pain felt every shift using foul smelling;
pain at the I in the surgical site. REEDA (Redness,
surgical site C Edema, Ecchymosis, b. absence of redness
Discharge, and itchiness;
P Approximation)
A ® frequent c. decreased pain felt in
T assessment can the surgical site.
T detect early signs
E and symptoms of
R infection.
N
4. Keep the area dry
and clean
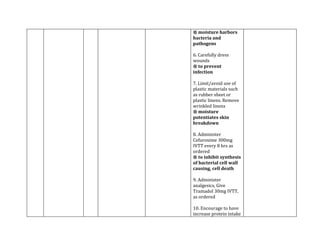
31.
® moisture harbors
bacteriaand
pathogens
6. Carefully dress
wounds
® to prevent
infection
7. Limit/avoid use of
plastic materials such
as rubber sheet or
plastic linens. Remove
wrinkled linens
® moisture
potentiates skin
breakdown
8. Administer
Cefuroxime 300mg
IVTT every 8 hrs as
ordered
® to inhibit synthesis
of bacterial cell wall
causing, cell death
9. Administer
analgesics, Give
Tramadol 30mg IVTT,
as ordered
10. Encourage to have
increase protein intake
32.
® to promotewound
healing
11. Encourage watcher
to provide patient with
appropriate vitamins
especially vitamin c
® to provide positive
nitrogen balance to
aid in skin/tissue
healing
33.
Date Cues Nee Nursing Objectives of Care Nursing Interventions Evaluation
/Ti d Diagnosis
me
F Subjective: C Acute Pain r/t That within our 3 1. Establish rapport to FEBRUARY 3, 2012
E “sakit kaayo O tissue injury s/t hour span of care, the patient as well as the
B akong likod” G surgical our patient will be significant others. @
R (referring to the N intervention able to decrease
U surgical site at I level of pain to 2. Note location of 3pm
A the back) T ® all cellular acceptable level as surgical procedures
R I damage caused evidenced by: ® as this can influence GOAL PARTIALLY
Y Objective: V by thermal, the amount of MET!
- Grimmace face E mechanical, or a. Decrease pain postoperative pain
3 noted - chemical stimuli scale from 3 to 1; experienced. After our 3 hour span
P results in the of care, our patient was
2 - Cries when E release of b. Absence or lessen 3. Monitor vital signs of able to decrease level
0 pain is felt R excitatory indicators of pain the patient of pain to acceptable
1 C neurotransmitte such as: grimaced ® changes in level as evidenced by:
2 - with Wong – E rs. Pain – face, crying, autonomic responses
Baker FACES P sensitizing irritability; may indicate increase a. Decreased pain scale
@ pain scale T substances in pain before the child from 3 to 1;
rating of 3 out 5 U surround the c. Vital signs within verbalizes.
12 where : A pain fibers in acceptable range. b. Lessen indicators
pm 0 – no pain L the extracellular 4. Observe non-verbal such as crying and
1 – 2 – mild fluid, creating cues (ex. facial irritability, although
pain P the spread of the expressions, guarding patient still exhibit
3 – moderate A pain message position, irritability, grimaced face;
pain T and causing restlessness)
4 – 5 – severe T inflammatory ® observations may or c. Vital signs of
pain E response. may not be congruent Temp – 36.7°C
R with verbal reports BP – 90/60 mmHg
- Irritability and N indicating need for PR – 100 bpm
restlessness further evaluation. RR – 28 cpm
noted
34.
5. Provide acalm and
- with vital quiet environment.
signs of:
Temp – 36.3°C 6. Provide distractions
BP – 100/60 or divertional
mmHG techniques when pain
PR – 117 bpm occurs such as: toys,
RR – 30 cpm music, reading stories
® distraction may help
the child divert his/her
attention to pain and
focus on another
object.
7. Give Tramadol 30mg
IVTT, as ordered
® to maintain
“acceptable” level of
pain.
8. Encourage significant
others to have the
patient adequate rest
periods.
® to prevent fatigue.
35.
Date Cues Nee Nursing Objectives of Care Nursing Interventions Evaluation
/Ti d Diagnosis
me
F Subjective: A Impaired Physical Within our span of 1. Establish rapport to FEBRUARY 8, 2012
E “Luya pa man C Mobility related care patient will the patient as well as the
B iyang lawas, T to Decrease maintain position of significant others. @
R sige lang siya I muscle strenght function and skin
U katulog, dili pa V secondary to Post integrity as 2. Monitor vital signs of 3pm
A pud siya kaayo I Operative evidenced by: the patient
R mag lihoklihok”, T Procedure - as baseline data GOAL MET!
Y as verbalized by Y 1.Absence of
grandmother - contractures 3. Determine diagnosis Within our span of
3 R 2.Absence of that contributes to care our patient was
Objective: E footdrop, and immobility discharged with
2 - Post operative S 3.Absence of - this will help to maintained position of
0 patient T decubitus identify the causative function and skin
1 - Slowed or contributing factors. integrity as evidenced
2 movement P by:
noted A 4. Observe movement
@ - Irritability T when client is unaware a. Absence of
noted T of observation contractures
12 - Flat on bed E - to note any b. Absence of
pm - Always asleep R incongruencies with footdrop, and
N reports of abilities. c. Absence of
- with vital decubitus.
signs of: 5. Support affected body
parts using pillows/rolls
- to maintain position
of function and reduce
risk of pressure ulcer
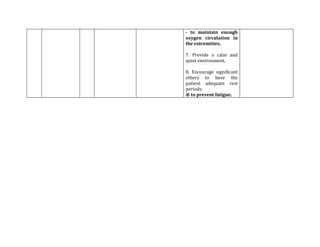
6. Assist in doing range
of motion
36.
- to maintainenough
oxygen circulation in
the extremities.
7. Provide a calm and
quiet environment.
8. Encourage significant
others to have the
patient adequate rest
periods.
® to prevent fatigue.
37.
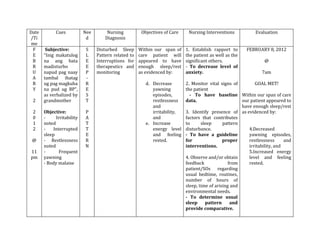
Date Cues Nee Nursing Diagnosis Objectives of Care Nursing Interventions Evaluation
/Ti d
me
F Subjective: N Risk for aspiration That within our 1. Note the level of FEBRUARY 3, 2012
E As verbalized by U r/t prescribed span of care, our consciousness of the
B the watcher: T position patient will be able patient @
R “kung paka-onon R to experience no
U nako siya, nag I aspiration as 2. Assess the ability of 3 pm
A higha gihapon T evidenced by: the child to swallow
R kay mao man gi I ® provides GOAL MET!
Y ingon sa doctor” O a. clear breath information about
N sounds, absence of potential for choking After our span of
3 Objective: A secretions in the or aspiration care, our patient was
- Patient flat on L mouth noiseless able to experience no
2 bed as ordered - respirations; 3. Auscultate lung aspiration as
0 M sounds before and evidenced by:
1 - on Diet as E b. have proper after feeding
2 tolerated with T feeding; ® to determine a. clear breath
strict aspiration A presence of sounds, absence of
@ precaution B c. watcher will secretions secretions in the
O identify risk factors mouth noiseless
7am - restlessness L of aspiration. 4. Instruct watcher to respirations;
noted I give semi-solid foods
C ® to aid swallowing b. had proper
- irritability noted efforts feeding;
P
A 5. Instruct watcher to c. watcher has
T feed patient slowly identified risk factors
T of aspiration.
E 6. Instruct watcher to
R give food when patient
N is not restless, not
talking or crying
38.
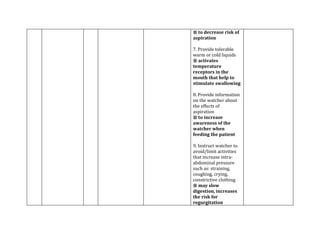
® to decreaserisk of
aspiration
7. Provide tolerable
warm or cold liquids
® activates
temperature
receptors in the
mouth that help to
stimulate swallowing
8. Provide information
on the watcher about
the effects of
aspiration
® to increase
awareness of the
watcher when
feeding the patient
9. Instruct watcher to
avoid/limit activities
that increase intra-
abdominal pressure
such as: straining,
coughing, crying,
constrictive clothing
® may slow
digestion, increases
the risk for
regurgitation
39.
Date Cues Nee Nursing Objectives of Care Nursing Interventions Evaluation
/Ti d Diagnosis
me
F Subjective: S Disturbed Sleep Within our span of 1. Establish rapport to FEBRUARY 8, 2012
E “Inig makatulog L Pattern related to care patient will the patient as well as the
B na ang bata E Interruptions for appeared to have significant others. @
R madisturbo E therapeutics and enough sleep/rest - To decrease level of
U napud pag naay P monitoring as evidenced by: anxiety. 7am
A tambal ihatag -
R ug pag magkuha R d. Decrease 2. Monitor vital signs of GOAL MET!
Y na pud ug BP”, E yawning the patient
as verbalized by S episodes, - To have baseline Within our span of care
2 grandmother T restlessness data. our patient appeared to
and have enough sleep/rest
2 Objective: P irritability, 3. Identify presence of as evidenced by:
0 - Irritability A and factors that contributes
1 noted T e. Increase to sleep pattern
2 - Interrupted T energy level disturbance. 4.Decreased
sleep E and feeling - To have a guideline yawning episodes,
@ - Restlessness R rested. for proper restlessness and
noted N interventions. irritability, and
11 - Frequent 5.Increased energy
pm yawning 4. Observe and/or obtain level and feeling
- Body malaise feedback from rested.
patient/SOs regarding
usual bedtime, routines,
number of hours of
sleep, time of arising and
environmental needs.
- To determine usual
sleep pattern and
provide comparative.
40.
5. Identify circumstances
thatinterrupt sleep and
frequency.
- To determine the
needs of adjustment.
6. Explain the necessity
of disturbances for
monitoring vital signs
and/or other care when
client is hospitalized
7. Arrange care to
provide for
uninterrupted periods
for rest, especially
allowing for longer
periods of sleep at night
when possible. Do as
much care as possible
without waking clients.
8. Provide quiet and
comfortable
environment.
- This will allow
patient to have longer/
enough rest period.
41.
PROGNOSIS
Factors Poor Fair Good Justification
1. Duration of Illness * The duration of illness, we rated it fair
because from the birth our patient already has
the condition. though he had undergone
surgical intervention at an early age.
2. Onset of Illness * The condition of the patient started after
birth, they noticed a mass bulging at the back.
At first they didn’t know what to do and were
afraid what might happen to it. They sought
medical attention and refused treatment at first
because of the lack of financial resources
3. Precipitating Factors * Since the cause of the disease is unknown,
and sometimes triggered during pregnancy. As
stated above, the mother during pregnancy was
noted avoid taking vitamins and supplements
during pregnancy.
4. Willingness to take * Despite the age of the patient. Commonly
the medication complaining of taking medications, still
complied with the aid of significant others to do
so as ordered by the physician.
5. Age * This condition is congenital and pediatric
patients are prone to this condition.
6. Environment * The environment is conducive to live. Free from
harm and pollutants.
7. Family Support * The grandmother of the patient is always there
to watch and support him, though his mother is
away from work they manage communicate
with the use of cellphone. His father also comes
to see him even though he is working hard to
support his son’s hospitalization.
42.
Computation: Rating Scale:
POOR –1 x 3 = 3 0 – 1.5 = Poor
FAIR – 2 x 2 = 4 1.6 – 2.0 = Fair
GOOD – 3 x 2 = 6 2.1 – 2.5 = Good
Total: 13 / 7 = 1.8 = FAIR
CONCLUSION:
We tallied and computed for the prognosis of the patient. Our patient has a fair
prognosis because they were able to seek medical and surgical attention at an early age and did
not wait for the condition to get worse. They are able and willing to comply the treatment
regimen given by the doctors. And the family is always there to support the patient. Also they
environment around the patient is good because he can play and interact with other people
without getting any disease or problems in the ward.
43.
DISCHARGE PLAN
Medication
Instructed to:
-Take the medications religiously
- Take the antibiotics with meals
- Take the medications on time without any lapses
- Educate the significant others about the drugs as well as its effect, indication, adverse effects
and what to do when it occurs
-Take home meds:
1. Cefixime 100mg/5ml 7 ml BID
2. Paracetamol 250mg/5ml 5ml q 4 hrs PRN for fever
Exercise
- Encourage to resume normal daily activities
- Encourage to exercise lower extremities by walking
-Encourage ambulation for faster recovery of damaged tissues
- Encourage passive range of motion exercises to strengthen muscles
Treatment
-Encouraged to follow the treatment regimen prescribed by the doctor
- Explain the significant others the importance of drug compliance
- Explain to the significant others, in their level of understanding, about the condition of the
patient
Hygiene
Encouraged to:
- Have daily hygiene
- Clean the surgical site and always keep it dry and clean
- Wash hands before and after eating and/or in contact with dirty objects
Out Patient Visit
- Instruct to return for follow up check up the OPD
- Instruct to monitor or watch closely for any unusuailties such as infections, bowel problems,
cough and colds, and report to their physician
Diet
- Instructed to continue to the usual diet
- Encouraged to eat foods rich in protein to aid in the healing of the wounds
- Encouraged to eat nutritious foods such as fruits and vegetables for faster growth and
development of the child
44.
RECOMENDATION
This case is interesting to us learners because the cause of this condition is still
considered unknown and still needs to be studied.
We recommend having further research and study of this case because there is more to
learn from this condition especially to us young nurses who still needs more knowledge and
experience. By exerting more effort and dedication we can help ourselves in this unending
quest for knowledge.