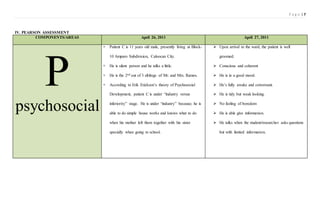
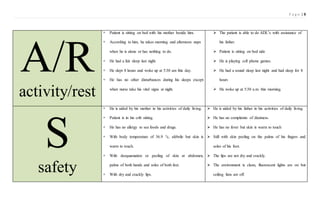
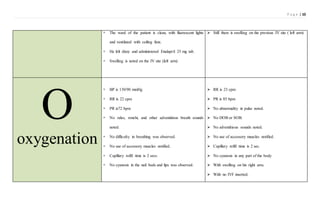
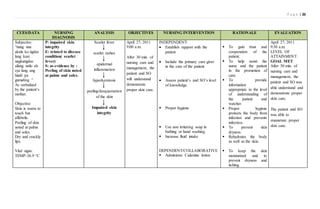
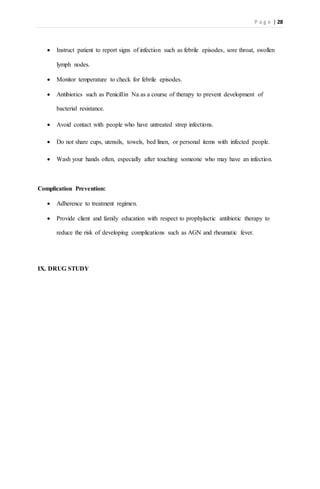
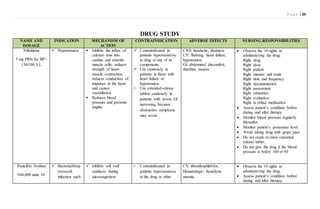
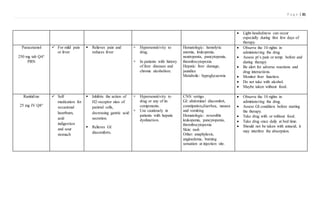
This document provides information on a case study of an 11-year-old male patient diagnosed with Scarlet Fever. It includes sections on introduction/background of Scarlet Fever, the patient's personal information and history, objectives of the study, nursing assessment using the PEARSON method, and daily updates on the patient's condition. The patient presented with a fever and rash and was initially diagnosed with atypical Kawasaki disease before the diagnosis was changed to Scarlet Fever. Nursing assessments focused on the patient's psychosocial, elimination, activity/rest, and other factors. The patient's condition was improving with treatment but he continued experiencing dizziness.