Downloaded 472 times

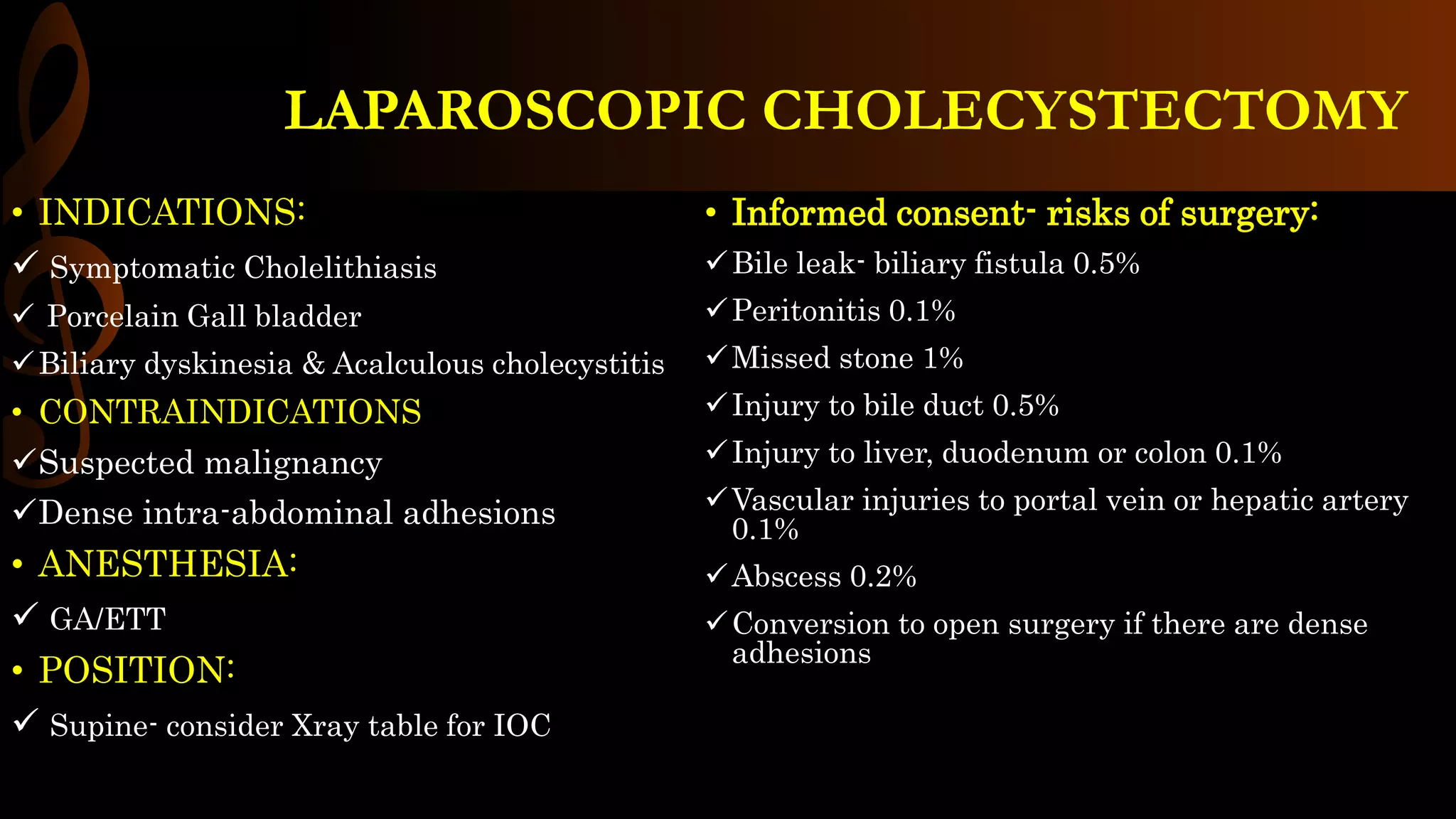



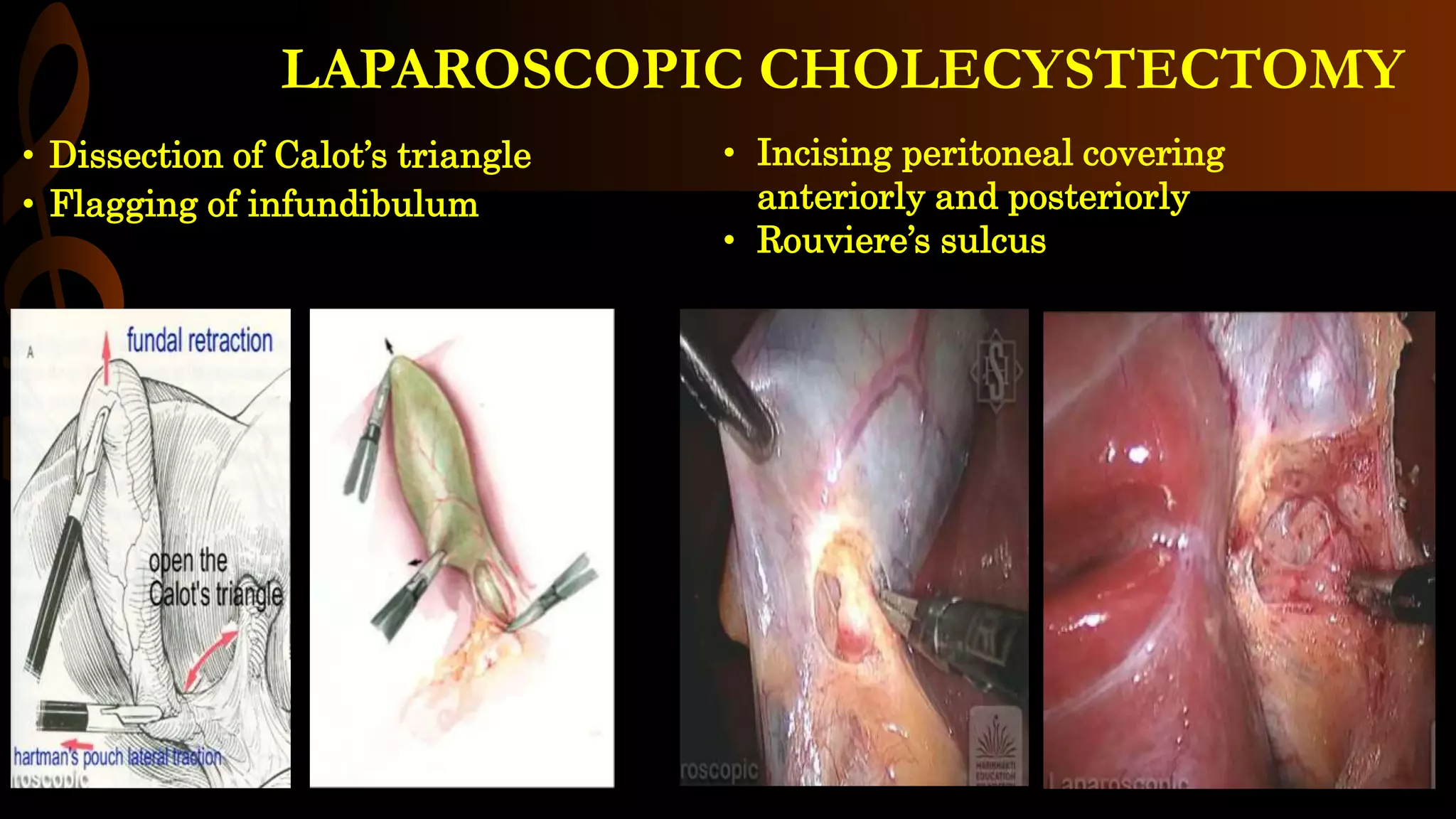

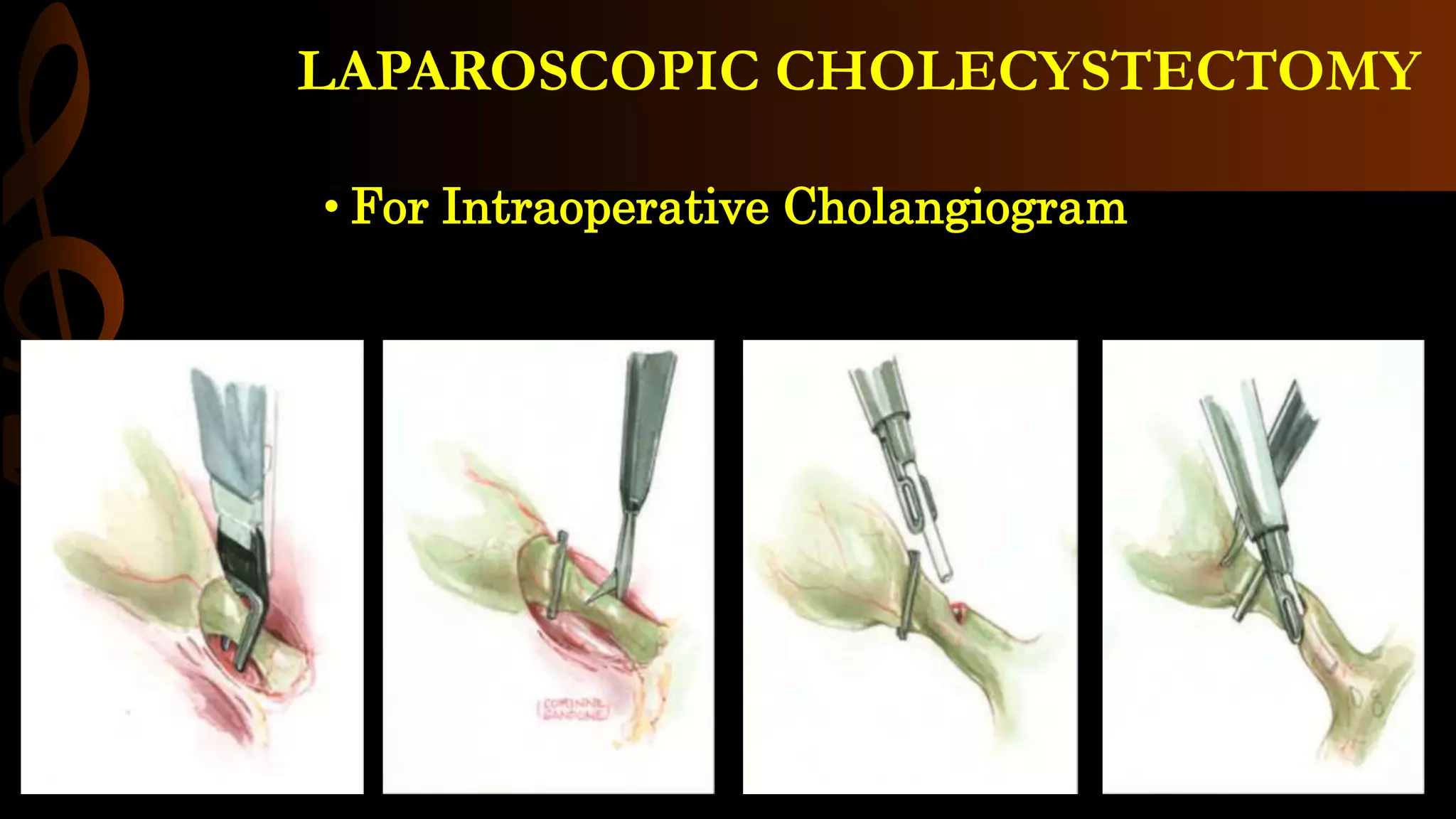





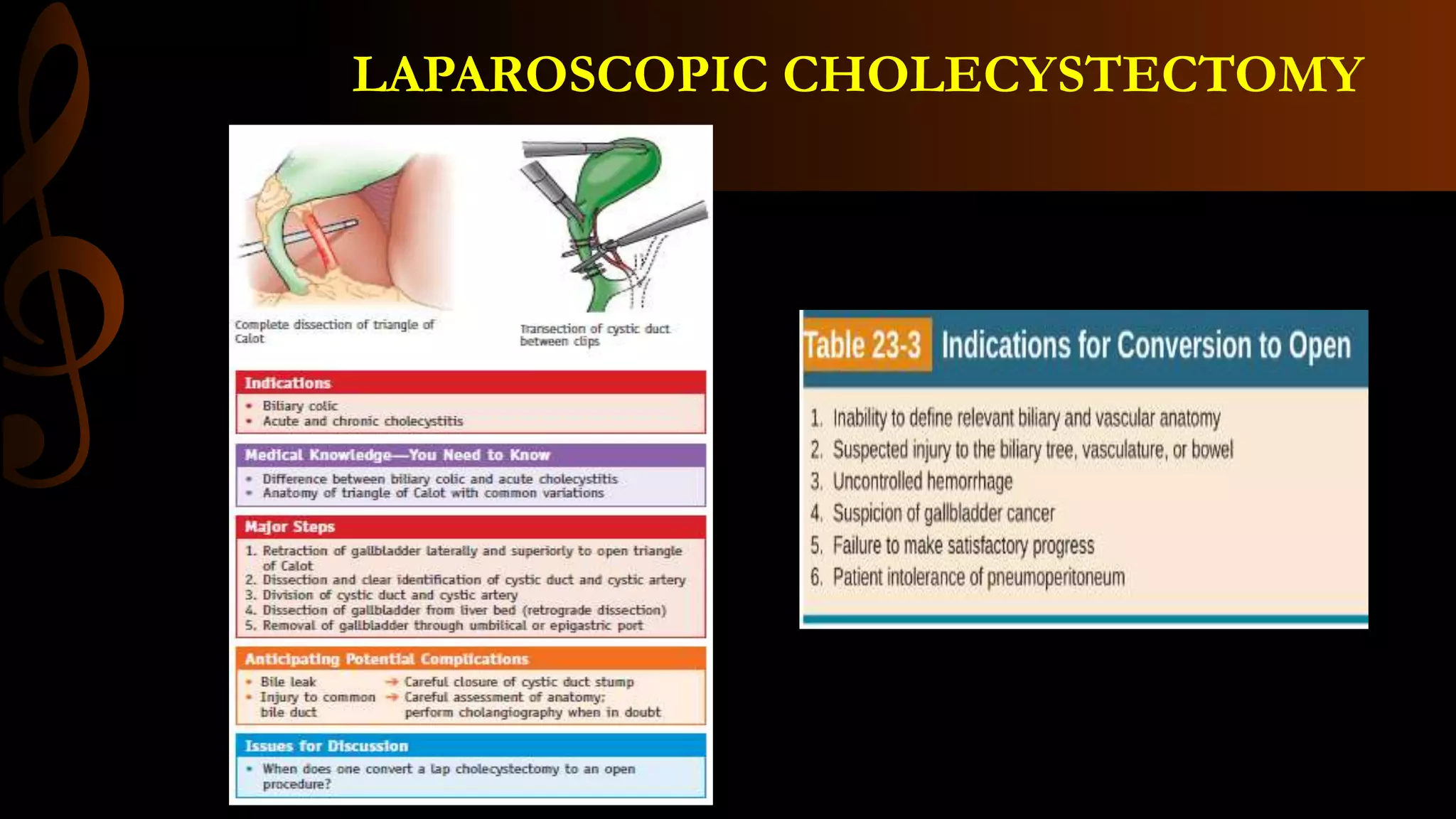


The document outlines the procedure for laparoscopic cholecystectomy, including indications, contraindications, anesthesia, positioning, surgical techniques, and post-operative care. It details the steps involved such as creating pneumoperitoneum, port placement, and critical views necessary for safe dissection. The risks associated with the surgery and the expected recovery timeline are also provided.























































































