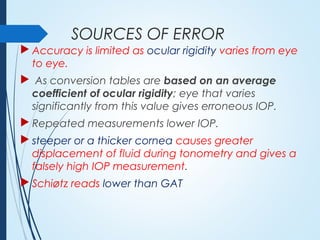
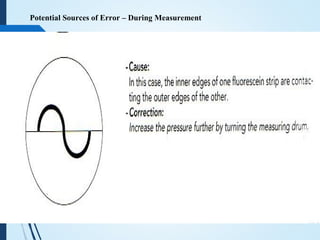
This document discusses the history and types of tonometry used to measure intraocular pressure (IOP). It describes various tonometers developed over time including Schiotz tonometry, the current gold standard Goldmann applanation tonometry, as well as other methods like indentation, non-contact, manometry and digital tonometry. Key details covered include the principles behind applanation and modified Imbert-Fick's law, calibration of tonometers, sources of error, advantages and limitations of different techniques.