BRVO
•Download as PPTX, PDF•
3 likes•1,025 views

Branched Retinal Vein Occlusion (BRVO) for undergraduate MBBS Students. Covers the basics of Aetiology, pathophysiology, clinical features, types, associated conditions and management of BRVO. Also encompasses salient points for PGMEE

Recommended
More Related Content
What's hot
What's hot (20)
Similar to BRVO
Similar to BRVO (20)
More from Abhishek Onkar
Recently uploaded
Recently uploaded (20)
BRVO
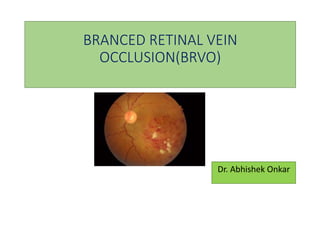
- 1. BRANCED RETINAL VEIN OCCLUSION(BRVO) Dr. Abhishek Onkar
- 2. Retinal Vein Occlusion • Retinal vein occlusion is the second most common cause of visual loss due to retinal vascular disease1-3 • Types: – Branch retinal vein occlusion (BRVO) – Hemi-retinal vein occlusion (HRVO) – Central retinal vein occlusion (CRVO) • BRVO is the most common3 – Five-year incidence of 0.6% (21/3558) for BRVO and – 3x m/c than CRVO3 • Persistent macular edema causes VA loss 1. Yau et al. Intern Med J. 2008; 2. RCO RVO guidelines. 2009; 3. Klein et al. Trans Am Ophthalmol Soc. 2000. HRVOBRVO 2
- 3. EPIDEMIOLOGY Definition : a segmental intraretinal haemorrhage not exceeding midline caused by obstruction in one of the branches of the main vein draining the corresponding retinal area first described by Leber in 1877 Age incidence : more than 90% cases >50yrs No sex/race predilection usually unilateral, bilateral only in 9% 3
- 4. CLASSIFICATION • one of the major branch retinal veins is occluded Major BRVO • one of the macular venules is occluded Macular BRVO 4 66% : Superotemporal quadrant
- 5. THEORIES OF AETIO-PATHOGENESIS 1.Arterio-venous Crossing 2.Degenerative Changes of Vessel Wall 3.Hematological Disorders 4.Resistance to Activated Protein C and Deficiency of Protein C or Protein S 5.Deficiency of Antithrombin and Mutation in the Prothrombin Gene 6.Anti-Phospholipid Antibodies and Hyperhomocysteinemia 5
- 6. Virchow’s triad Hemo- dynamic changes (venous stasis) Degenerative changes of vessel wall Blood hyper- coaguability 6
- 7. Systemic risk factors associated with retinal vein occlusion Hypertension, hyperlipidemia, diabetes mellitus Atherosclerotic vascular disease: coronary artery disease, high BMI, smoking Neoplasia: polycythemia rubra vera, multiple myeloma, leukemia Vasculitis: systemic lupus erythematosus, sarcoid, syphilis Drugs: oral contraceptives, diuretics Ocular risk factors include glaucoma and hyperopia 7
- 8. Pathogenesis of Macular Edema in BRVO Vascular occlusion/hypoxia Increased VEGF / IL-6 secretion damage to the tight junctions of capillary endothelial cells BRB Breakdown Fluid flux from vessels to tissue according to Starling's law 8
- 9. BRVO : C/F Major BRVO • can be asymptomatic or • with visual blurring usually involving the sector of visual field corresponding to the area of the retina involved. Macular BRVO • there is always a central visual disturbance with normal peripheral vision •asymptomatic/Sudden painless loss of Vn •Vision loss at presentation is related to the extent of macular damage from intraretinal oedema, haemorrhage or capillary non-perfusion 9
- 10. OPHTHALMOSCOPIC FEATURES Acute RVO Chronic RVO Intra-retinal haemorrhages : flame shaped & dot - blot Cystoid macular edema Hard exudates RPE atrophy Cotton wool spots ERM / sheathing of vessels Optic disc edema Shunt vessels/ venous collaterals Macular edema NVD/NVE/NVI Dilated , tortuous retinal veins in segmental distribution Late complications : VH RD NVG 10
- 11. Infero-temporal brvo in female aged 53years : dilated , tortuous veins. soft exudates and hemorrhages 11
- 12. Sheathed ST - VEIN 12
- 13. NV at macula 13
- 14. a sheathed supero temporal vein. Haemorrhages and cotton wool spots in supero-temporal acute BRVO 14
- 15. The characteristic fluorescein angiographic findings in BRVO include ACUTEPHASE • Delayed venous filling/emptying • Areas of Capillary non- perfusion/closure : • A. Perfused BRVO— <5DD • B. Non-perfused BRVO : >5DD • Macular oedema : perfused, non- perfused or mixed LATEPHASE • micro vascular abnormalities • Late staining and leakage from the affected veins is seen • particularly useful in determining the extent of ME and Ischemia • Blocked fluorescence d/t hemorrhages seen through all phases • Dilated capillaries, microaneurysms and telangiectatic changes seen 15
- 16. Blocked fluorescence & non-perfusion Late staining Leakage around blocked vessel late staining 16
- 17. NV and ME 17
- 18. OCT imaging ME in IT-BRVO L/E 18
- 19. SYSTEMIC W/U 19
- 20. W/U of patients with venous obstruction (age>50 years) Disorder Investigation Hypertension B.P. Diabetes F.B.S CVA DUPLEX-U/S ECG Hyperlipidemia LIPID PROFILE Temporal arteritis ESR CRP CBC 20
- 21. Algorithm for investigations in RVO 21
- 22. TREATMENT MODALITIES T/T MODALITIES 1. Anti- aggregative therapy and firbrinolysis 2. Isovolemic hemodilution 3.Sheathotomy & vitrectomy 4. Intravitreal & periocular steroids 5. Intravitreal VEGF inhibitors 6. Laser therapy 22
- 23. • Current treatment options focus on the sequelae of the occluded venous branch, such as ME, NV, VH , TRD . • The complex pathogenesis of this disease requires investigation and treatment of all risk factors (hypertension, diabetes mellitus, blood lipid disorders, hematological disorders). 23
- 24. Intravitreal Corticosteroids • In various studied doses from 4 to 25 mg, triamcinolone acetonide (TA) has been reported to be effective • complications are raised intra-ocular pressure, infectious endophthalmitis, post-injection steroid-induced cataract, retinal detachment. 24
- 25. OZURDEX™ (dexamethasone intravitreal implant) • OZURDEX® : FDA-approved t/t for macular edema following BRVO. • Injectable, biodegradable intravitreal implant contains 0.7 mg (700 μg) dexamethasone in NOVADUR™ solid polymer DDS (preservative-free). preloaded in sterile, single-use, applicator • Poly (D,L-lactide-co-glycolide) PLGA biodegradable polymer matrix : slowly degrades to lactic acid and glycolic acid as dexamethasone is gradually released. 25
- 26. ANTI-VEGF AGENTS : MOA 26
- 27. Humanized monoclonal IgG antibody against VEGF-A 1.25 to 2.5 mg monthly x 6 months Off-label use M/c a/e : conjunctival hyperemia and subconjunctival hemorrhage at injection site. 1.BEVACIZUMAB (AVASTIN) 27
- 28. 2.RANIBIZUMAB ( LUCENTIS ) Fab fragment of parent molecule of bevacizumab Designed for intra-ocular use.FDA approved 0.5 or 0.3 mg monthly x 6months 10-25 x more costly 28
- 29. Macular Grid Laser Photocoagulation MLG is recommended as an effective treatment to reduce the ME in BRVO : after a period of 3 to 6 months after onset and following absorption of the majority of hemorrhage if VA is 20/40 or worse. If FFA reveals macular nonperfusion, MLG not warranted. Argon MLG is usually used for this purpose. However, diode laser (810 nm) and krypton red laser (647 nm) also can be used. 29
- 30. Applied only to the area of leaking capillaries cover all areas of leaking capillaries within 2 DD of fovea not extend beyond 2DD from fovea not extend within the FAZ avoid collateral vessels and retinal haemorrhages 100 µm spots at 0.1 second produce medium white burn •spacing of one half to one burn-width apart 30
- 31. Scatter Laser Photocoagulation significantly reduced the development of retinal neovascularization and vitreous hemorrhage. if all eyes with large retinal nonperfusion were treated, 64% of these patients would never develop NV. If only the eyes that develop NV were treated, the events of VH decrease from 61% to 29%. waiting is generally advocated until NV actually develops before scatter photocoagulation is considered. 31
- 32. Laser spots spaced one burn width apart covering entire involved segment extending no closer than 2 DD from fovea Spot Size : 200-500 microns Duration : 0.1 s Medium white burn Argon green/ Ag blue- green 32
- 33. Clinical Trials and Venous Occlusive Diseases 2010 Anti-VEGF Ranibizumab studies BRAVO and CRUISE 2009 Steroid studies SCORE Study Ozurdex Trials Laser studies 1980s Branch Vein Occlusion Study (BVOS) 1990s Central Vein Occlusion Study (CVOS) 33
- 34. • Perform FA for macular edema, macular non-perfusion, retinal neovascularization only after retinal hemorrhages have cleared adequately (3-6 months) • If macular edema is the cause of a vision less than 6/12, undertake macular grid photocoagulation. • If macular non-perfusion is the cause of decreased vision then no laser treatment should be performed. Follow up these cases every four months. • If retinal non-perfusion more than 5 disc areas, follow up for neovascularization at 4 monthly intervals. • Undertake laser photocoagulation in the involved quadrant only if neovascularization develops. BVOS 34
- 35. BRVO Summary BRVO: • SCORE: Laser better than IVTA • OZURDEX: Dexamethasone better than sham (no laser arm) • BRAVO: Ranibizumab monthly for 6 months better than observation/laser in BRAVO. Improved VA: 61% vs 29% eyes gained 15 or more letters 35
- 36. T/T summary in RVO’s T/T Modality CRVO BRVO Erythrocyte/platelet anti- aggregative therapy Routine use of ticlopidine / troxerutine for improving VA or resolution of VH not recommended Fibrinolysis Limited use in acute CRVO (<11days): I.V. low dose rt- PA +Heparin Routine use not recommended Isovolemic hemodilution Routine use for improving VA or resolution of VH not recommended Pars plana vitrectomy Routine use not recommended Intra-vitreal steroids Improve VA /resolve ME TA not sup. to MLG. A/E >than MLG /anti- VEGF Intra-vitreal anti-VEGF Bevacizumab/ranimizumabused effectively for improving VA , resolving ME & NV.Trials ongoing. 36
- 37. Modality CRVO BRVO Grid laser photocoagulation Not recommended for t/t of ME Indicated in ME and VA≤20/40 of 3 months duration. Not recommended in macular ischemia . Scatter laser photocoagulation For NV : prophylactic t/t not recommended if gonioscopy & dilated fundus examination possible every 4 weeks . If NV +nt : prompt laser to avoid sec. complications Recommended if disc / retinal NV +nt 37
- 38. Natural Course and Visual Prognosis Determine the natural course of BRVO efficiency of the developing collateral circulation integrity of arterial perfusion to the affected sector Site/degree of occlusion, 38
- 39. In general, BRVO has a good prognosis. 50–60% of eyes have a final VA of 20/40 or better even without any treatment. Chronic ME and VH d/t neovascularizations account most frequently for a poor final VA. Retinal neovascularization and persistent ME develop in 25% and 60% of eyes, respectively. 39