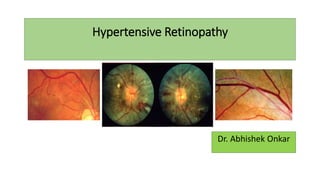
Hypertensive Retinopathy
•Download as PPTX, PDF•
3 likes•855 views

Hypertensive Retinopathy (HTN-R) for undergraduate MBBS Students. Covers the basics of Aetiology, pathophysiology, clinical features, Classification and management of HTN-R. Also encompasses salient points for PGMEE

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hypertensive Retinopathy
Similar to Hypertensive Retinopathy (20)
More from Abhishek Onkar
Recently uploaded
Recently uploaded (20)
Hypertensive Retinopathy
- 2. Hypertensive retinopathy • Hypertensive retinopathy refers to retinal microvascular signs that develop in response to raised blood pressure. • Prevalence: 4-10% (UK) • Signs of hypertensive retinopathy are frequently seen in adults 40 years and older, and are predictive of incident stroke, congestive heart failure, and cardiovascular mortality—independently of traditional risk factors. • major risk factor for the development of other retinal vascular diseases, such as retinal vein and artery occlusion, and ischaemic optic neuropathy. • increases the risk of both development of diabetic retinopathy and its progression. • Adequate control of blood pressure reduces vision loss associated with DR. • Only essential (primary) and malignant hypertension are relevant to the discussion of hypertensive retinopathy.
- 3. RISK Factors
- 4. • Retinal arteries are histologic arterioles with 100 µm calibers and no internal elastic lamina or continuous muscular coat. Changes in the luminal diameter of the arterioles are the most important component in regulating systemic arterial blood pressure. • Retinal arterioles and capillaries are similar in anatomy to cerebral vessels in that they exhibit autoregulatory mechanisms and tight junctions to maintain the blood-ocular barrier. • Vasoconstriction can be regarded as an autoregulatory attempt to control the volume of blood received by the retinal capillary bed. • Choroidal arterioles and capillaries have fenestrations (ie, no blood-ocular barrier) and do not exhibit autoregulation. • Optic nerve–head vessels exhibit intermediary characteristics with autoregulation but an incompetent blood-ocular barrier as a result of the peripapillary choroidal vessels. • Because of the vascular differences between the retina, the choroid, and the optic nerve, each of these anatomic regions responds differently to hypertension. Together, however, they represent the clinical picture of the ocular response to systemic hypertension.
- 5. Hypertensive vascular changes • Arteriosclerotic changes are chronic changes resulting from systemic hypertension. In the retina, atherosclerosis and arteriolosclerosis predominate. • According to Spencer, the normal light reflex of the retinal vasculature is formed by the reflection from the interface between the blood column and vessel wall. [1] • Initially, the increased thickness of the vessel walls causes the reflex to be more diffuse and less bright. (broadened arteriolar reflex)
- 6. • Progression of sclerosis and hyalinization causes the reflex to be more diffuse and the retinal arterioles to become red-brown. This is known as copper wiring. • Advanced sclerosis of the retinal vasculature leads to increased optical density of the retinal blood vessel walls; this is visible on ophthalmoscopy as a phenomenon known as sheathing of the vessels. • When the anterior surface becomes involved, the entire vessel appears opaque (pipestem sheathing). The patency of such vessels has been demonstrated by fluorescein angiography. • When sheathing encircles the wall, it produces a silver-wire vessel
- 7. • Generalized attenuation of the arterioles results from diffuse vasospasm, which occurs when a significant elevation of blood pressure has persisted for an appreciable period. (normal A-V ratio =2:3) • A relationship has been noted between the narrowing of the caliber of the arteriole and the height of the diastolic pressure. • Increased intraluminal pressure either in the retinal arterioles or in the central artery of the retina causes narrowing of the arterioles. • Focal arteriole narrowing was closely related to control of hypertension (Wang et al) and was the precursor to more recognized microvascular abnormalities associated with hypertension. [2] • Focal narrowing occurs from spasm of local areas of the vascular musculature or from edema in and around the vessel wall, which can become permanent with fibrosis
- 8. • In arteriovenous nicking (the Gunn sign), impeded circulation results in a dilated or swollen vein peripheral to the crossing, causing hourglass constrictions on both sides of the crossing and aneurysmal-like swellings. • Arteriovenous (AV) nicking is the hallmark of hypertensive retinopathy Hypotheses: Thickening of the basement membrane and the media of the arteriole in hypertension impinge on the vein and cause the crossing phenomenon (Ikui). [1] Mimatsu: due to sclerotic thickening of the wall of the venule and not by compression by the arteriole Seitz: attributed the crossing phenomenon to vascular sclerosis and perivascular glial cell proliferation and not to venous compression. [1]
- 9. • Sclerosis may shorten or elongate retinal arterioles, with the branches coming off at right angles. This change in length deflects the veins at the common sheath and changes the course of the vein (Salus sign). • According to Albert et al, the original crossing angle, the degree of vascular thickening, and the pressure differential influence this phenomenon. • Bonnet sign: Dilatation/Banking of the distal portion of the vein, in an arteriovenous crossing.
- 11. Symptoms ointermittent blurring oGradual painless loss of vision oVisual field defect oheadache and red face: indicating accelerated/malignant hypertension. oSudden painless loss of vision: HTN- related CRVO/CRAO/BRVO oPainful loss of vision: high IOP d/t NVG subsequent to CRVO oIsolated oculo-motor nerve palsy is unusual feature of hypertension. It accounts for approximately 30% of acquired diplopia (sixth nerve most commonly) and usually resolves spontaneously within 3 months.
- 12. CHRONIC HYPERTENSIVE RETINOPATHY • Usually asymptomatic. • Narrowing and irregularity of retinal arteries • Arteriovenous nicking (narrowing of retinal veins at arteriovenous crossing sites) • Blot retinal hemorrhages • Microaneurysms Associated features: Branch retinal vein occlusion ■ Central retinal vein occlusion ■ Macroaneurys
- 13. DIFFERENTIAL DIAGNOSIS OF CHRONIC HYPERTENSIVE RETINOPATHY • Diabetic retinopathy • Retinal venous obstruction • Hyperviscosity syndromes • Congenital hereditary retinal arterial tortuosity • Ocular ischemic syndrome • Radiation retinopathy
- 14. MALIGNANT ACUTE HYPERTENSIVE RETINOPATHY • Symptoms: headache, scotoma, diplopia, decreased vision, and photopsias. • Clincial findings are divided into three distinct categories: retinopathy, choroidopathy, and optic neuropathy. • constriction of arterial vascular beds from the release of circulating catecholamines. • Retinal hemorrhages • Cotton-wool spots • Serous retinal detachment • Optic disc edema Associated features ■ Choroidal ischemia ■ Retinal pigment epithelial changes ■ Optic neuropathy ■ Proteinuria, stroke, kidney failure, encephalopathy
- 15. DIFFERENTIAL DIAGNOSIS OF ACUTE HYPERTENSIVE RETINOPATHY • Bilateral central retinal vein obstruction • Bilateral bullous central serous chorioretinopathy • Collagen vascular diseases • Diabetic retinopathy (especially in the setting of diabetic papillopathy) • High altitude retinopathy
- 17. Classification • Examination of the fundi with use of the Keith– Wagener–Barker classification for hypertensive retinopathy can be helpful in assessing both the duration and the severity of the hypertension and had prognostic implication on survival. • demonstrated that, at that time, hypertensive patients with grade 4 retinopathy had a 3 year survival rate of 6%, as opposed to a survival rate of 70% in those with grade 1 retinopathy . • Nowadays, funduscopy still plays a major role in the management and risk stratification of hypertensive patients: The ESH/ESC 2007 Guidelines consider hypertensive retinopathy grade 3 and 4 as target- organ damage
- 18. CLASSIFICATION • No classification is satisfactory because of the high variability of clinical findings. • studies show that features correlate poorly with severity of hypertension, and may be seen in individuals without hypertension, occurring in up to 10% of adults • Documentation of elevated blood pressure is more valuable than any classification system.
- 19. Prognostic significance • Recent studies evaluating fundus findings and their relation to systemic disease, such as the Blue Mountains Eye Study, the Atherosclerosis Risk in Communities (ARIC) Study, the Multi-Ethnic Study of Atherosclerosis, and the Beaver Dam Eye Study concluded: • There is solid evidence that signs of advanced hypertensive retinopathy, such as isolated micro-aneurysms, haemorrhages, hard exudates, and cotton-wool spots, are strongly associated with subclinical cerebrovascular disease and predict stroke, coronary artery disease, congestive heart failure, and cardiovascular mortality, independently of blood pressure and other traditional risk factors
- 20. Keith-Wagener-Barker classification (1939) • Patients were grouped according to their ophthalmoscopic findings. As such, this was the first system to correlate retinal findings with the hypertensive disease state. • Group 1 - Slight narrowing, sclerosis, and tortuosity of the retinal arterioles; mild, asymptomatic hypertension • Group 2 - Definite narrowing, focal constriction, sclerosis, and AV nicking; blood pressure is higher and sustained; few, if any, symptoms referable to blood pressure • Group 3 - Retinopathy (cotton-wool patches, arteriolosclerosis, hemorrhages); blood pressure is higher and more sustained; headaches, vertigo, and nervousness; mild impairment of cardiac, cerebral, and renal function • Group 4 - Neuroretinal edema, including optic disc edema; Siegrist streaks, Elschnig spots; blood pressure persistently elevated; headaches, asthenia, loss of weight, dyspnea, and visual disturbances; impairment of cardiac, cerebral, and renal function
- 21. Keith-Wagener-Barker Classification Grade 1 Grad 2 Grade 3 Grade 4 • Arteriolar narrowing + + + + + + + + + + • Arteriovenous nicking + ++ + + + • Retinal haemorrhages + + + • Micro-aneurysms + + + • Hard exudates + + + • Cotton-wool spots + + + • Optic disc swelling + • Macular oedema +
- 24. Mitchell-Wong simplification of the Keith- Wagener-Barret system Grading • Grade 1 (mild retinopathy) - Arteriolar narrowing (generalized and focal), AV nicking, and/or arteriolar wall opacity • Grade 2 (moderate retinopathy) - Hemorrhage, microaneurysm, cotton wool spot, and/or hard exudate • Grade 3 (malignant retinopathy) - Moderate retinopathy plus optic disc swelling
- 29. Management • History • Duration of HTN • B.P.: MOST IMPORTANT • Past glycemic control (hemoglobin A1c) • Medications • Systemic history (e.g., obesity, renal disease, DM, serum lipid levels, pregnancy) • Ocular history
- 30. Examination • Visual acuity • Measurement of IOP • Gonioscopy when indicated (for neovascularization of the iris or increased IOP) • Slit-lamp biomicroscopy • Dilated fundoscopy: Hypertensive retinopathy is a clinical diagnosis made when characteristic retinal vascular, choroidal or optic disc changes are visualized on fundoscopy/slit-lamp biomicroscopy.
- 31. Ophthalmic Investigations • Fundus Photography • Fluorescein Angiography to: guide treatment to identify Ischemic areas • Optical Coherence Tomography: o Retinal thickening assessment oMonitoring of edema o vitreo macular traction • USG – B scan: when media unclear d/t dense cataract or VH
- 32. PREVENTION • Prevention- targeting modifiable risk factors/ lifestyle modifications
- 33. Treatment • Anti-hypertensives: strict control of B.P. • Intravitreal ANTI- VEGF: MACULAR EDEMA (Bevacizumab, Ranimibizumab) • LASERS: RETINOPATHY (argon green) • RETINAL DETACHMENT SURGERY: RD • VITRECTOMY: VH