Presentation1, radiological imaging of slipped femoral capital epiphysis.
•Download as PPTX, PDF•
14 likes•2,257 views

health&medicine

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological imaging of slipped femoral capital epiphysis.
Similar to Presentation1, radiological imaging of slipped femoral capital epiphysis. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of slipped femoral capital epiphysis.
- 1. Radiological imaging of Slipped Capital Femoral Epiphysis. Dr/ ABD ALLAH NAZEER. MD.
- 2. Slipped capital femoral epiphysis (SCFE), is a relatively common condition affecting the physis of the proximal femur in adolescents. It is one of commonest hip abnormalities in adolescence and is bilateral in ~20% of cases. Epidemiology SUFE is more common in boys than girls and more common in Afro-Caribbeans than Caucasians. The age of presentation is somewhat dependent on gender with boys presenting later (10-17 years) than girls (8-15 years). Obesity is a significant risk factor. Clinical presentation Patients present with hip pain progressing to a limp and even leg length discrepancy. If SUFE is confirmed on an X-ray, the child should be rested, admitted and not allowed to weight-bear. Pathology SUFE is essentially a type I Salter-Harris growth plate injury due to repeated trauma on a background of mechanical and probably hormonal predisposing factors. Conditions that may predispose to SUFE include: hypothyroidism hypopituitarism hyperparathyroidism
- 3. Plain radiograph AP and frog-leg: the commonest situation allows assessment of two views In the pre-slip phase, there is a widening of the growth plate with irregularity and blurring of the physeal edges and demineralization of the metaphysis. This is followed by the acute slip which is posteromedial. In a chronic slip, the physis becomes sclerotic and the metaphysis widens (coxa magna). The slip that occurs is posterior and to a lesser extent medial, and therefore is more easily seen on the frog-leg lateral view rather than the AP hip view. Because the epiphysis moves posteriorly, it appears smaller because of projectional factors. On the AP, a line drawn up the lateral edge of the femoral neck (line of Klein) fails to intersect the epiphysis during the acute phase (Trethowan's Sign). The metaphysis is displaced laterally, and therefore may not overlap posterior lip of the acetabulum as it should normally (loss of triangular sign of Capener).
- 4. Ultrasound: Ultrasound may be performed in the assessment of hip pain. However, it should not be used as a replacement for a pelvic radiograph. Findings are nonspecific and may include hip joint effusion. In some cases, malalignment of the femoral epiphysis and metaphysis may be seen. CT: CT is a sensitive and an accurate method of measuring the degree of upper femoral epiphyseal tilt and detecting the disease in its early stage. Multiplane reconstruction allows assessment of the relationship of the femoral head to the metaphysis in three planes. However, the dose required for the examination means that it should not be used unless absolutely necessary. The metaphyseal blanch sign described increases in the density of the proximal metaphysis. It represents an attempt of the healing process that occurs before the visible displacement of the epiphysis. MRI: In the acute stage, marrow edema results in increased signal on T2-weighted sequences, e.g. STIR. Marrow edema is non-specific, and while it may indicate early bone changes in SUFE, there are numerous other causes, e.g. infection or tumour. MRI can be used to examine the contralateral hip which is important because of the high incidence of bilateral slip. STIR: high signal in epiphysis and metaphysis joint effusion T1: low signal in edematous regions metaphyseal displacement
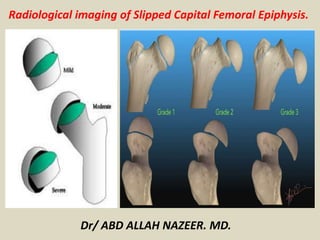
- 8. Radiographic Findings in SCFE • Klein’s Criteria (1951) • Earliest: Widened and irregular growth plate, compared to contralateral hip Increased lucency medially • Angulated contour of femoral head, then becomes rounded with adaptation • Periosteal proliferation at inferior, posterior margins and further slippage create “crow’s beak” • Klein's Line • Line drawn along superior border of femoral neck should cross at least a portion of the femoral epiphysis (Klein, 1951) • Most sensitive indicator of a mild slip on plain film Classification Grade I: displacement of epiphysis less than 30% of width of femoral neck Grade II: slip between 30%-60% Grade III: includes slips of greater than 60% the width of neck
- 13. Radiographs showed subtle widening of the physis on the right side on anteroposterior view, (a) posterior and medial displacement of the epiphysis of the right femur with respect to femoral neck on lateral (b) and frog's lateral view (c)
- 14. Bilateral slipped capital femoral epiphysis. One side shows evidence of remodeling of the neck and an anterior bone bump that restricts flexion. The other side demonstrates an acute slip as seen by the absence of any evidence of remodeling.
- 16. SLIPPED CAPITAL FEMORAL EPIPHYSIS.
- 19. Coronal TI-WI (a) and T2-WI (b) magnetic resonance imaging images reveals physeal widening with indistinct margins and adjoining bone marrow edema
- 20. Axial TI-WI (a), T2-WI (b), Sagittal TI-WI (c) and T2-WI (d) magnetic resonance imaging images reveal posterior and medial displacement of femoral capital epiphysis with respect to metaphysis with physeal widening with indistinct margins and adjoining bone marrow edema.
- 21. Slipped capital femoral epiphysis.
- 23. Slipped capital femoral epiphysis Coronal T1 (1a), coronal fat-suppressed T2 (1b), sagittal fat- suppressed proton density (1c) and axial fat-suppressed T2 (1d) weighted images.
- 25. Thank You.