Downloaded 218 times
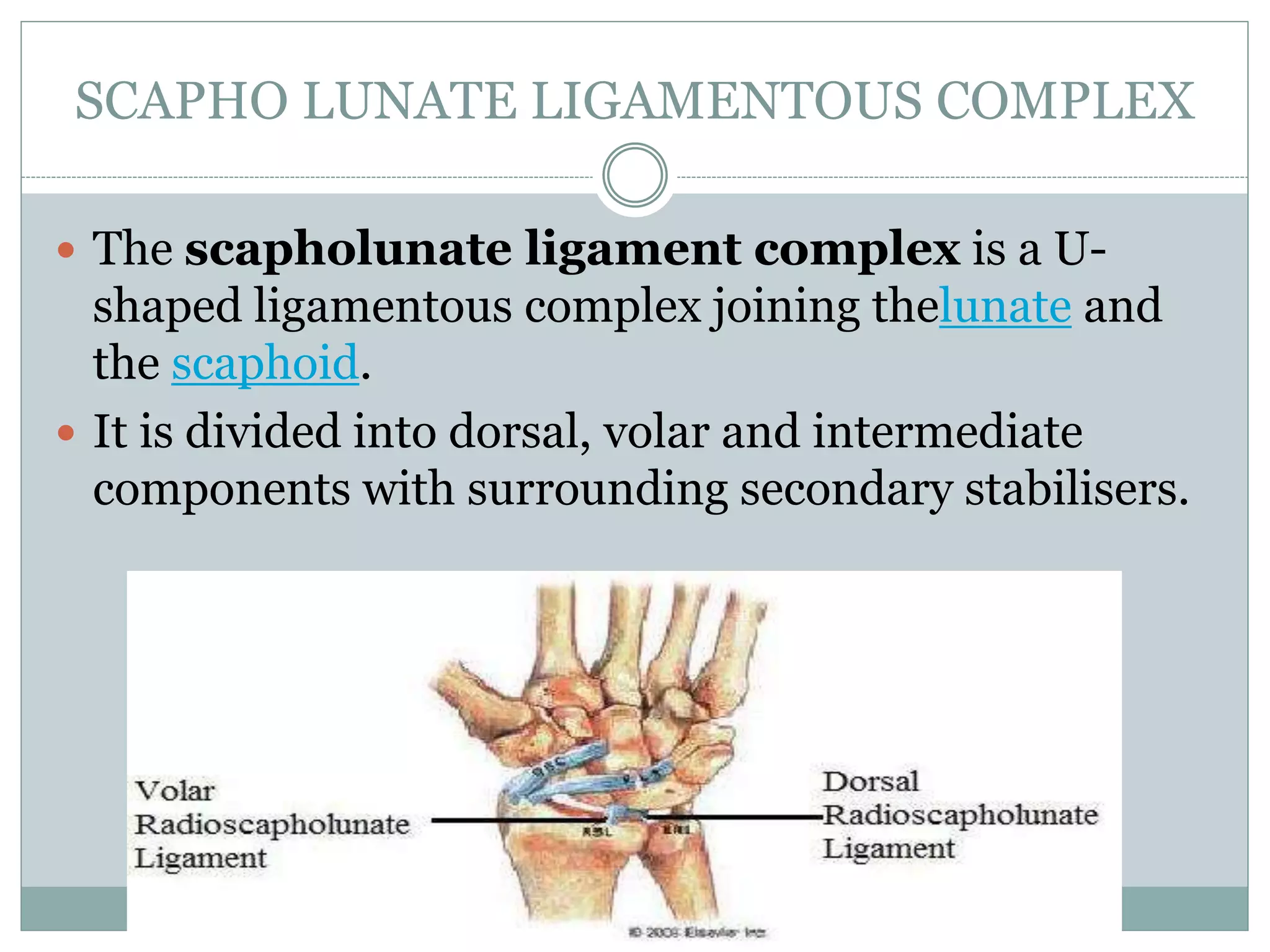










This document discusses scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC), two common patterns of post-traumatic wrist arthritis. It describes the etiology, anatomy, radiographic features, classifications, effects on joint kinematics, differential diagnosis, and treatment options for both conditions. Surgical treatments include four-corner arthrodesis, capitolunate arthrodesis, scaphoidectomy, proximal row carpectomy, and complete wrist arthrodesis. Both SLAC and SNAC can lead to abnormal joint motion and progressive degenerative arthritis if left untreated.












































































