Downloaded 26 times

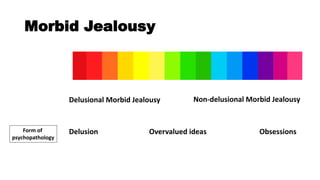





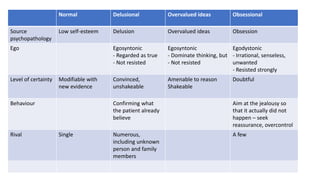


This document discusses morbid jealousy and its subtypes. It defines jealousy as a negative emotional response to a threatened relationship, and morbid jealousy as an unfounded preoccupation with a partner's infidelity. Morbid jealousy can be delusional, involving false beliefs despite evidence, or non-delusional, involving obsessions and compulsive behaviors. Theories for its development include psychodynamic, cognitive, and social factors. Assessment considers diagnoses like delusional disorder or obsessive-compulsive disorder. Treatment focuses on underlying psychopathology through psychotherapy and medication management.















































![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)
![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)






![Kesejahteraan Emosi di Tempat Kerja [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/kesejahteraanemosi2020-200905072541-thumbnail.jpg?width=640&height=640&fit=bounds)






























